A pharmacy claim can look clean and still be wrong. That is the uncomfortable truth employers need to understand. A drug can pass through adjudication, meet the plan’s coverage rules, generate a paid claim, and still fail the most important test: whether that medication is appropriate, necessary, and likely to work for the patient.
Clinical rigor is the discipline that closes that gap.
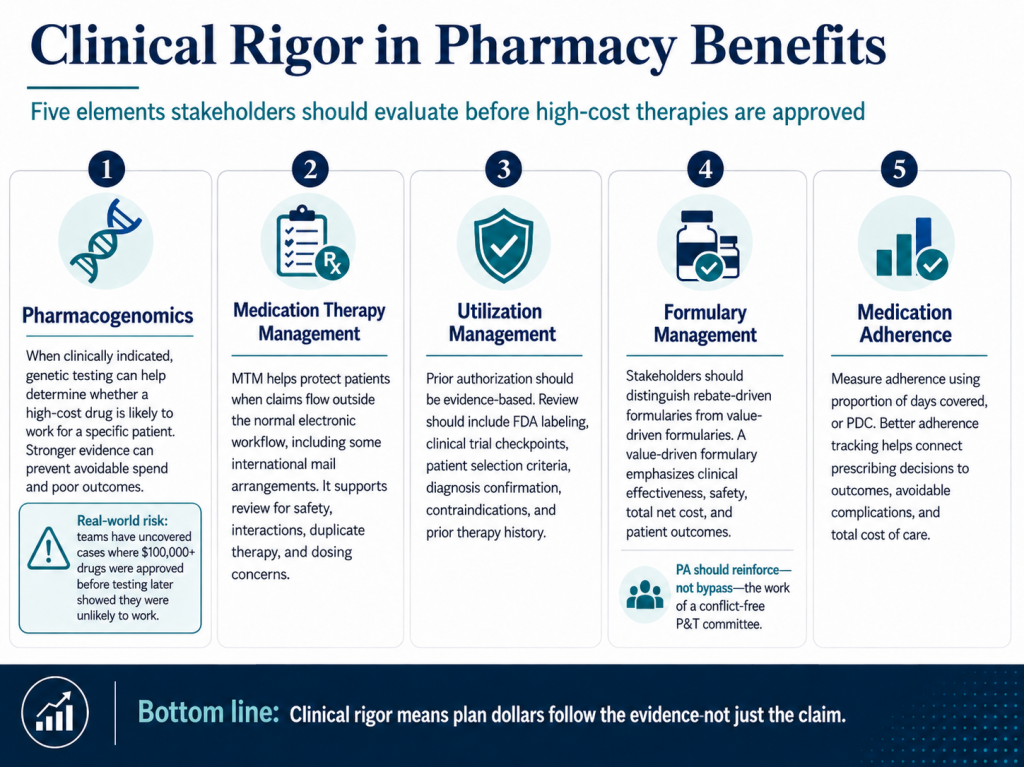
Over the past 10 years, while onboarding new clients, our team has identified dozens of situations where drugs costing more than $100,000, per year, had already been adjudicated and approved, only for genetic testing to later reveal they were unlikely to work for the patient. That is not a minor oversight. It is a break in the evidence trail before plan assets were spent.
The key elements include:
- Pharmacogenomics gives employers and fiduciaries another layer of clinical protection. It can help determine whether a patient’s genetic profile makes a drug ineffective, unsafe, or less appropriate than another therapy. Pharmacogenomics is not relevant to every drug or every patient, but where it is clinically indicated, it should be part of the review before a high-cost approval. For high-cost therapies, especially specialty medications, this should not be treated as academic medicine. It is practical plan governance.
- Medication therapy management is just as important. This becomes even more critical when plans use international mail programs or when claims adjudicate outside the normal electronic workflow. When a claim bypasses the standard drug utilization review process, the plan may also lose basic clinical safeguards, including checks for duplicate therapy, drug-drug interactions, contraindications, and dosing concerns. A lower unit cost is not a bargain if clinical oversight is stripped out of the transaction.
- Utilization management must also carry real clinical weight. Prior authorization should not be a paperwork ritual. A credible PA process should review FDA labeling, clinical trial checkpoints, patient selection criteria, diagnosis confirmation, contraindications, and prior therapy history. The question should not be, “Was the form completed?” The question should be, “Does this patient match the evidence that supports use of this drug?”
- Formulary management is where fiduciary discipline often gets tested. Employers should know the difference between a rebate-driven formulary, which may favor drugs that improve PBM economics and a value-based formulary, which weighs clinical effectiveness, safety, total net cost, and patient outcomes. But even a sound formulary can be undermined if a conflict-free P&T committee’s evidence-based decisions are bypassed by rubber stamped prior authorizations. The PA process should defend the formulary’s clinical logic, not quietly dismantle it.
- Medication adherence is the last piece, and it is often the most measurable. Plans should track proportion of days covered, or PDC, to understand whether members are actually taking their medications as prescribed. Poor adherence turns good prescribing into poor outcomes and can drive avoidable medical spend.
Clinical rigor is not about slowing care down.
It is about refusing to let plan dollars move faster than the evidence. For employers with fiduciary responsibilities, that distinction matters. A pharmacy benefit should not merely pay claims. It should prove, before and after payment, that the therapy was worth funding.
How We Can Work Together
Whether you’re a plan sponsor trying to get control of pharmacy spend, or a broker guiding clients through PBM decisions, education is the fastest way to improve outcomes. If you want a focused, high-value session your team can actually use, here are several ways we can work together.
Option 1: Get Certified
American College of Benefit Specialists (ACoBS) equips benefits professionals with practical knowledge across pharmacy, medical, retirement, and voluntary benefits. Organizations working with ACoBS-certified consultants gain better plan oversight, stronger vendor accountability, and more disciplined cost control. The certification signals a clear commitment to fiduciary guidance and protecting plan assets.
Option 2: Book a Webinar
A clean, educational session for employers, brokers, or TPAs. We’ll cover the most common PBM profit tactics, how to spot contract red flags, and what a fiduciary standard of care looks like in pharmacy benefits. Great for client education and thought leadership.
Option 3: Join the Virtual Roundtable
Bring your internal team (HR, Finance, and Benefits) or your broker group. I’ll lead a live discussion focused on PBM oversight, cost drivers, and what to ask your PBM right now. You’ll leave with a short action list you can use immediately.
Option 4: Get a Quote
Pharmacy benefits now rival medical spend for many plans. Yet most are still governed by contracts few have fully read and pricing models few can clearly explain. That is a fiduciary risk, not just a cost issue.
If you want lower spend, tighter oversight, and alignment you can defend in front of a board or audit committee, act with intent. Certify your team. Educate your clients. Pressure test your PBM.