Group Purchasing Organizations (GPOs) often market their rebate aggregator programs as tools to deliver greater savings through scale. These structures can create opaque rebate spreads that inflate costs for plan sponsors while enriching intermediaries. Employers and consultants who understand how these spreads form and how to counter them can protect their plans from hidden markups.
1. Avoid Use of Rebate Aggregator Formularies
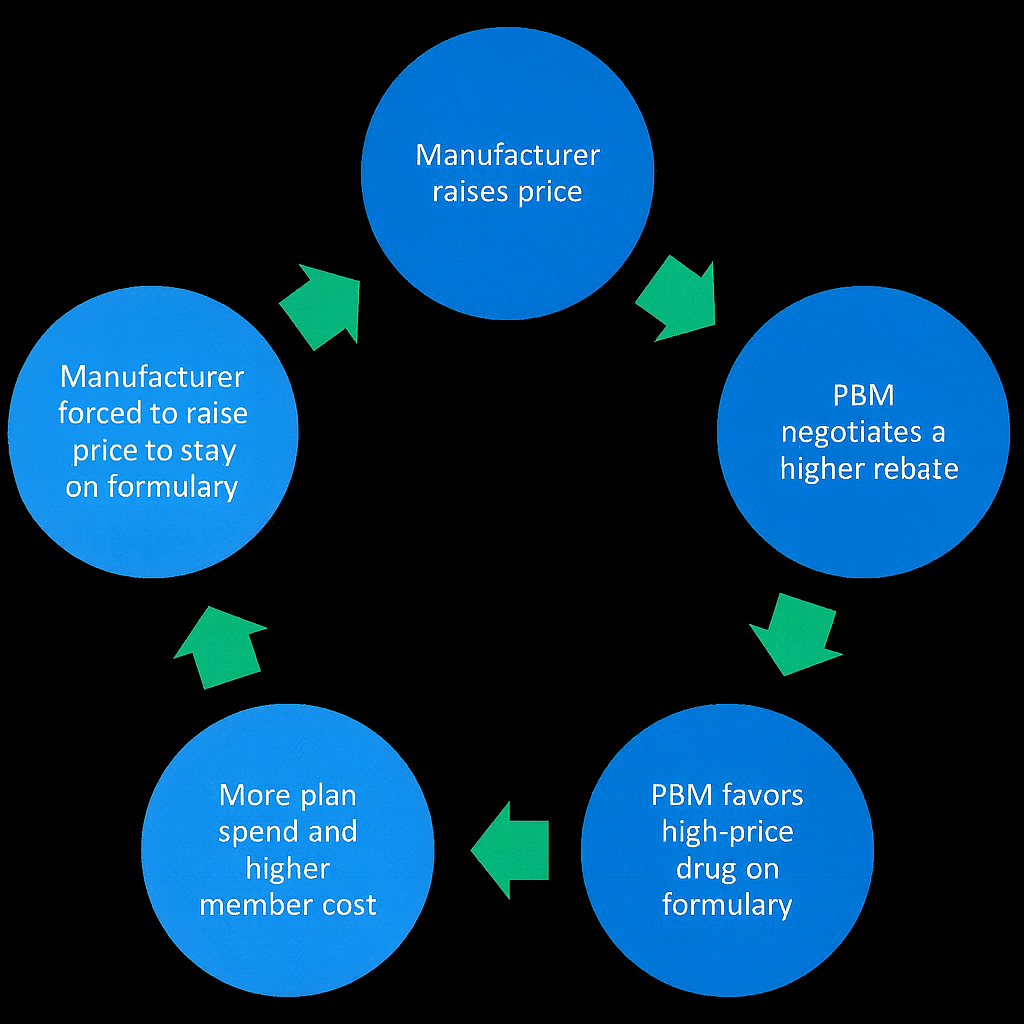
A rebate aggregator formulary is a prepackaged drug list built around maximizing rebates instead of minimizing net cost. These formularies are typically managed by the GPO or its contracted PBM and emphasize drugs that deliver high rebate dollars rather than clinical or financial efficiency.
For example, an aggregator might favor a brand drug that pays a $200 rebate even though a generic alternative costs $300 less per fill. While the GPO and PBM split the rebate revenue, the plan sponsor ultimately pays more in total net cost.
Trade-offs
- Pros: Larger rebate checks and a perception of “shared savings.”
- Cons: Weaker clinical oversight, higher net plan costs, and misaligned incentives where formulary placement favors rebate-rich drugs instead of clinically superior or lower-cost options.
Better Approach
Employers can insist on an independent formulary managed under a fiduciary PBM model. This ensures that rebate and formulary decisions are made based on clinical value and lowest net cost, not the PBM’s or aggregator’s revenue objectives. Fiduciary PBMs contractually commit to passing through 100 percent of rebates and disclose all revenue sources, giving employers full visibility into pricing and rebate flow.
2. Achieve a 91% – 93% Generic Dispense Rate (GDR)
A high Generic Dispense Rate (GDR) directly limits rebate spread opportunities. Rebate spreads thrive on brand utilization; every time a brand is dispensed over a clinically equivalent generic, the PBM or aggregator earns more rebate margin while the plan sponsor pays more.
When a plan consistently dispenses generics, especially in chronic care categories such as hypertension, cholesterol, and mental health, the volume of high-rebate brand claims falls, shrinking the room for rebate manipulation.
How to Improve GDR
- Formulary design: Exclude brands where a generic is clinically appropriate.
- Real-time benefit tools: Give prescribers visibility into cost-effective alternatives during prescribing.
- Member engagement: Communicate savings opportunities through digital nudges, pharmacist counseling, and plan education.
Key Takeaway
Chasing rebates at the expense of GDR is a losing strategy. A plan with 91% GDR and minimal rebates will nearly always outperform a plan with 85% GDR and “big rebate guarantees.” A higher GDR means fewer rebate-driven brand drugs and a cleaner, more efficient drug spend while maintaining the access needed for better health outcomes.
3. Limit Eligibility Exclusions That Undermine Rebate Access
PBMs and aggregators often use technical exclusions to withhold rebates that should belong to the plan. Common tactics include coding claims as “Dispense As Written” (DAW) or using step therapy rules that push a claim outside the rebate-eligible definition.
Example
Suppose a plan member fills a high-cost brand drug coded as DAW 1, meaning the prescriber requested no substitution. If the PBM’s rebate contract defines this as “non-rebate eligible,” the plan loses the rebate even though the PBM still collects it from the manufacturer. That difference becomes spread revenue.
Countermeasures
- Tight contract language: Define rebate eligibility broadly to include all formulary brand claims, regardless of DAW or utilization management flags.
- Audit regularly: Review rebate remittance reports and identify discrepancies between paid claims and rebate payments.
- Reconcile quarterly: Require detailed rebate reconciliations comparing manufacturer invoices to plan-level data to prevent leakage.
These measures ensure that the plan, not the PBM or aggregator, captures the full rebate value generated by its members’ utilization.
Final Thoughts
Employers must stop measuring PBM performance by rebate guarantees and start focusing on net cost integrity. Rebate aggregator models often convert transparency into opacity, masking spreads that work against plan sponsors. By rejecting rebate-driven formularies, driving generic use, and policing rebate eligibility, employers can regain control of their pharmacy spend and align incentives with their fiduciary duty. The best defense against rebate spreads is not a bigger rebate. It is a transparent, data-driven PBM relationship that prioritizes the plan’s financial and clinical outcomes over rebate revenue.
If you are a director of benefits seeking more control and clarity in your pharmacy program, TransparentRx can help you achieve it with confidence. As a fiduciary PBM, we align our interests with yours to deliver accountability, measurable savings, and better outcomes for plan members. Learn how our fiduciary approach supports informed decision-making and long-term value. Schedule a brief discovery call to explore how transparency can strengthen your benefit strategy.