4 questions to ask before signing your next PBM service agreement [Weekly Roundup]
4 questions to ask before signing your next PBM service agreement and other notes from around the interweb:
- 4 questions to ask before signing your next PBM service agreement. The very idea of managing pharmacy benefits might make you nauseous. That’s because drug prices are skyrocketing, creating significant challenges for your company’s bottom line. You may think that your pharmacy benefit manager (or PBM) – who is responsible for handling contractual relationships between drug manufacturers, health insurance providers, pharmacies, and patients – would negotiate the best possible deals for everyone involved. Unfortunately, recent reports from the PBM Accountability Project show otherwise: PBMs often misuse their immense power by adding secret streams of revenue for themselves. The Federal Trade Commission (FTC) has noted this trend too and announced plans in 2022 to investigate the inner workings of PBMs. But some states are taking it upon themselves to crack down on PBM business dealings, too. For example, Florida and Iowa joined Michigan in passing legislation in 2022 that regulates certain PBM practices – while Ohio’s Medicaid department is also conducting audits.
- Lawsuit Challenges Federal Copay Accumulator Policy. On August 30, 2022, a coalition led by the HIV and Hepatitis Policy Institute filed a new lawsuit in federal district court in DC to challenge a Trump-era policy that allows insurers and pharmacy benefit managers (PBMs) to not apply financial support from a drug manufacturer towards a patient’s deductible or annual out-of-pocket maximum. If an insurer or PBM adopts such a policy, the enrollee cannot “count” a copay or other drug manufacturer coupon—typically used to help reduce patient costs at the pharmacy counter—towards a patient’s overall annual out-of-pocket costs. This policy was adopted in May 2020 in the final 2021 notice of benefit and payment parameters and has not been altered since. More than two years later, the plaintiffs argue that this policy is unlawful because it conflicts with the Affordable Care Act (ACA), is inconsistent with other agency regulations, and is arbitrary and capricious under the Administrative Procedure Act. They ask the court to set aside this policy. The timing of the lawsuit may be designed to influence the forthcoming proposed 2024 notice of benefit and payment parameters, which is expected later this year.

- How specialty drug ‘solution stacking’ can rein in pharmacy benefit costs. Brokers and employer groups alike know that 5% to 10% percent of insured workers and their dependents drive 50% to 60% of the cost of pharmacy claims. A few members with prescriptions for a specialty drug with a five-figure price tag can easily represent most of an entire group’s pharmacy spend. These drugs are often lifesaving or provide a dramatic quality of life improvement for those who take them. No one would question the necessity of using them. But when a group can mitigate some of the cost without affecting the clinical outcome, it can be a game changer. The broker who unlocks these savings becomes a trusted ally.
- Senate Bill and FTC 6(b) Study Turn the Heat on Pharmacy Benefit Managers Amid Drug Pricing Concerns. Introduced on May 24, 2022, the Pharmacy Benefit Manager Transparency Act of 2022 is a bipartisan bill co-sponsored by Senators Maria Cantwell (D-WA) and Charles Grassley (R-IA) that imposes compulsory disclosure requirements on PBMs while seeking to limit certain controversial PBM practices such as spread pricing. The Act also empowers the FTC and state attorneys general to take enforcement action against PBMs that engage in “unfair and deceptive acts” or “dissemination of false information” related to PBM services. The proposed legislation expressly prohibits three types of controversial PBM activities that may be considered “unfair or deceptive,”4 including: (1) Charging a health plan or payer a different sum for a prescription drug’s ingredient cost or dispensing fee than the PBM reimburses a pharmacy for the prescription drug’s ingredient cost or dispensing fee, then retaining the difference as profit, a practice known as “spread pricing.”


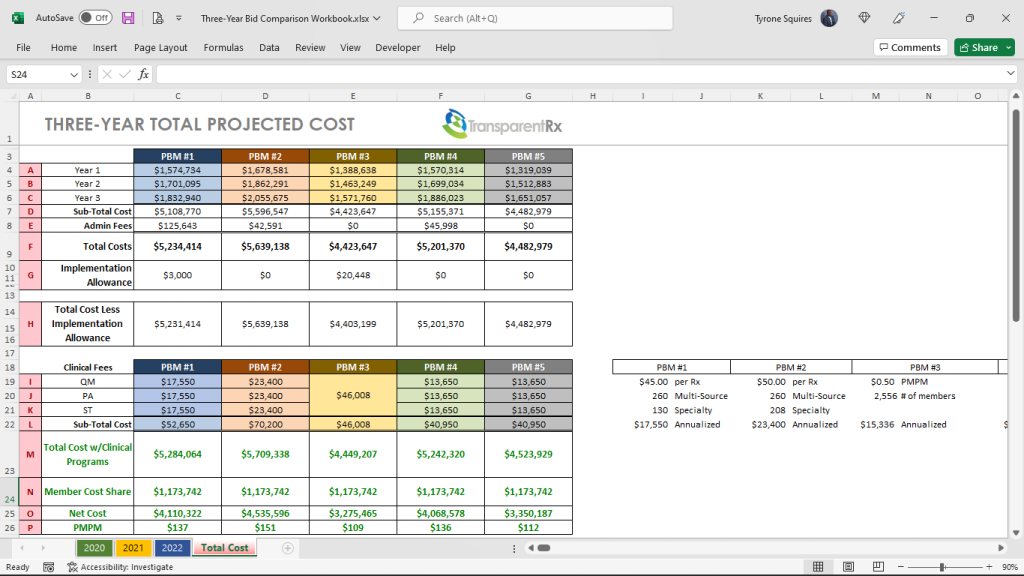
 Once all bids are collected the consultant then plugs them into their in-house Excel spreadsheet or a third-party bid analyzer software platform. This is where the problems begin more on that in a bit.
Once all bids are collected the consultant then plugs them into their in-house Excel spreadsheet or a third-party bid analyzer software platform. This is where the problems begin more on that in a bit.