Tuesday Tip of the Week: Factor Benefit Design into your PBM Scorecard (Rerun)
Factor in the actual benefit design, not questions about benefit design, into your PBM scorecard. At a minimum, it should be the same form the PBM uses to set your group up in the back-office. Sometimes even the PBM’s benefit design form excludes important details, such as DAW codes, so be careful. If important information is missing get it included especially when that information contributes to your cost.
 |
| Click to Learn More |
Never once during hundreds of RFPs has any consultant or broker ever asked us for a signature ready benefit design as part of our response. I’ve not taken a poll so I don’t know the reason. Maybe it is because some believe benefit design doesn’t have a big role in determining cost. If that is the case, nothing could be further from the truth. I would be asking for a benefit design to be submitted as if we were going live with it.
Don’t put 50 questions in a RFP around benefit design where important details get lost in translation. Instead, get a copy of a signature ready benefit design and score it as part of the PBMs proposal. Here are some weights I recommend applying to each scorecard:
Contract – 40%
Benefit Design – 25%
References – 10%
Questionnaire – 5%
Reverse Auction – 15%
Finalist Presentation – 5%
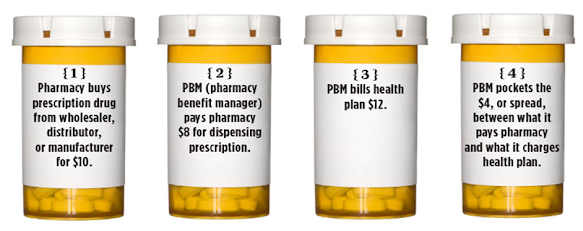
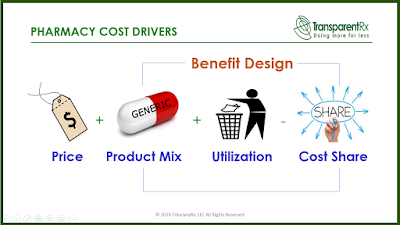
In pharmacy cost drivers, price is 1A and benefit design is 1B. Aside from copayments and deductibles (cost sharing) most plan sponsors know little else about their benefit design and have left it up to the PBM to decide. When the PBM is non-fiduciary that could lead to significant overpayments.