
Reference Pricing: “Gross” Invoice Cost vs. AWP for Popular Generic and Brand Prescription Drugs (Volume 328)
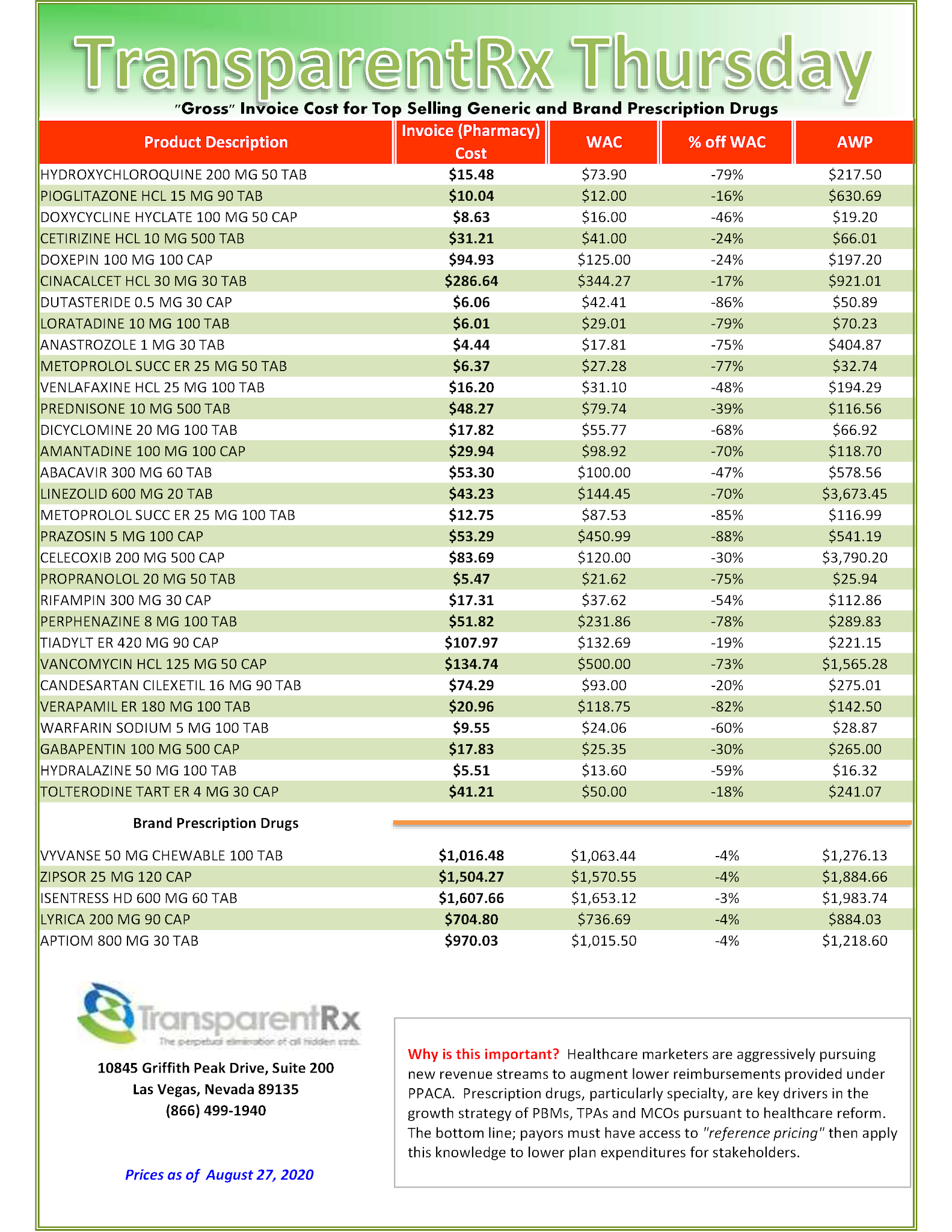
Step #4: Now take it one step further. Check what your organization has paid, for prescription drugs, against our acquisition costs then determine if a problem exists. When there is more than a 5% price differential for brand drugs or 25% (paid versus actual cost) for generic drugs we consider this a potential problem thus further investigation is warranted.
Multiple price differential discoveries mean that your organization or client is likely overpaying. REPEAT these steps once per month.
— Tip —
Tuesday Tip of the Week: Out-of-pocket caps don’t lead to increased health plan spending or reduced affordability for all enrollees
Investigators noted that not enough is known about the effects of caps on patient costs, and they sought to remedy this deficit via their study. They noted that specialty drugs such as antiviral agents for hepatitis C and biologic agents for multiple sclerosis or rheumatoid arthritis are highly effective but spending for these agents is disproportionate to that for other drugs.
By the Numbers
“Over the past decade, health-plan spending for such treatments increased from an estimated 26% of total drug spending to 49%, while the treatments remained below 2.5% of total prescriptions dispensed,” they wrote.
Meanwhile, the use of high cost-sharing drug tiers among employer sponsored health plans has risen from 11% to 51%, with a simultaneous increase in the disparity in OOP spending between specialty drug users and nonspecialtiy drug users, “becoming 3 times as large as that in an earlier 10-year period,” the authors wrote.
In just the past 2 years, at least 21 states and the federal government have introduced legislation to control OOP patient costs for prescription drugs, and 11 states have introduced laws targeting specialty drug spending. Of the latter group, Delaware, Louisiana, and Maryland passed legislation and imposed caps on OOP for commercial health plans at $150 per 30-day supply of specialty medication, the authors wrote.
Free Webinar | The Untold Truth: How Pharmacy Benefit Managers Make Money
The reason so many PBMs are reluctant to offer radical transparency is in doing so their revenues would be cut in half! How many businesses do you know will voluntarily cut their revenues in half? Instead, non-fiduciary PBMs seek out arbitrage opportunities to foster top-line growth. Want to learn more?

“Thank you! Awesome presentation.” Mallory Nelson, PharmD
“Thank you Tyrone for this informative meeting.” David Wachtel, VP
“…Great presentation! I had our two partners on the presentation as well. Very informative.” Nolan Waterfall, Agent/Benefits Specialist
A snapshot of what you will learn during this 30-minute webinar:
- Hidden cash flow streams in the PBM Industry
- Basic to intermediate level PBM terminologies
- Examples of drugs that you might be covering that are costing you
- The #1 metric to measure when evaluating PBM proposals
- Strategies to significantly reduce costs and improve member health
Sincerely,
TransparentRx
Tyrone D. Squires, MBA
10845 Griffith Peak Drive, Suite 200
Las Vegas, NV 89135
866-499-1940 Ext. 201
P.S. Yes, it’s recorded. I know you’re busy … so register now and we’ll send you the link to the session recording as soon as it’s ready.
Reference Pricing: “Gross” Invoice Cost vs. AWP for Popular Generic and Brand Prescription Drugs (Volume 327)

Step #4: Now take it one step further. Check what your organization has paid, for prescription drugs, against our acquisition costs then determine if a problem exists. When there is more than a 5% price differential for brand drugs or 25% (paid versus actual cost) for generic drugs we consider this a potential problem thus further investigation is warranted.
Multiple price differential discoveries mean that your organization or client is likely overpaying. REPEAT these steps once per month.
— Tip —
Tuesday Tip of the Week: Factor Benefit Design into your PBM Scorecard
 |
| Click to Learn More |
Pharmacy CEO pleads guilty to $50M reimbursement fraud
Central Rexall Drugs was paid more than $50 million in reimbursements from pharmacy benefits managers from 2015 to 2016, according to Mr. Carpenito. He also said Ms. Taff, who will be sentenced Dec. 1, received more than $1.5 million from the scheme.
Recruiters told the patients which medications to get based on how much reimbursement the pharmacy would receive from insurance companies for the drugs, not because the patients needed them, Mr. Carpenito said. The drugs covered within these New Jersey workers’ insurance plans included expensive pain, antifungal, scar and libido medications with reimbursements that often ran as high as thousands of dollars per month, WNBC reported.
 |
| Click To Learn More |
Tyrone’s Commentary:
The PBMs were likely involved with uncovering the fraud still it should not have gone this far but why? Many if not most of those reimbursed drugs should have been excluded from the formulary in the first place. Shame on the PBMs for pushing these claims through by rubberstamping prior authorizations and plan sponsors for signing off on what is more than likely an open or some sort of hybrid formulary which allowed those claims to be adjudicated. You can’t “keep employees happy” to the extent you run an inefficient pharmacy benefit program. It doesn’t matter how much money you have to throw at a pharmacy expenses. If it isn’t managed cost-effectively it is a failure. All PBMs are not created equally. My PBM, TransparentRx, scrutinizes every single claim at the same time maintaining CFO satisfaction scores hovering around 90%. For those who believe PBMs are an unneccessary expensive, you get a birds-eye view of a future without us.
Hayley Taff, CEO of Hammond, La.-based pharmacy Central Rexall Drugs, pleaded guilty Aug. 12 to playing a key role in a scheme that garnered more than $50 million in false reimbursements. Ms. Taff and her co-conspirators recruited public employees in New Jersey to get pricey specialty prescriptions they had not been prescribed, according to U.S. Attorney Craig Carpenito of the District of New Jersey.
Reference Pricing: “Gross” Invoice Cost vs. AWP for Popular Generic and Brand Prescription Drugs (Volume 326)
This document is updated weekly, but why is it important? Healthcare marketers are aggressively pursuing new revenue streams to augment lower reimbursements provided under PPACA. Prescription drugs, particularly specialty, are key drivers in the growth strategies of PBMs, TPAs, and MCOs pursuant to health care reform.
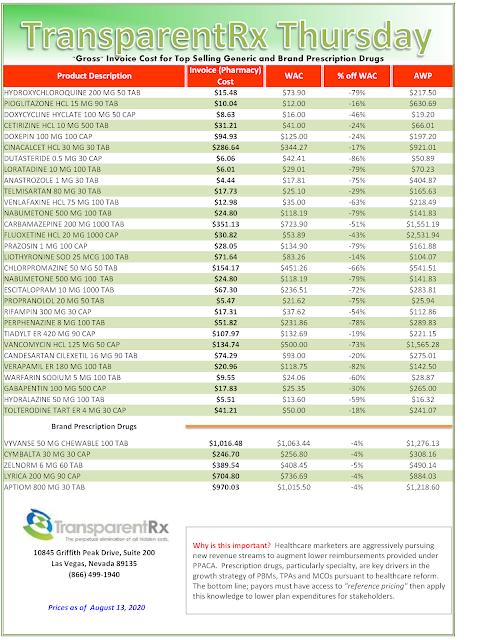
Step #4: Now take it one step further. Check what your organization has paid, for prescription drugs, against our acquisition costs then determine if a problem exists. When there is more than a 5% price differential for brand drugs or 25% (paid versus actual cost) for generic drugs we consider this a potential problem thus further investigation is warranted.
Multiple price differential discoveries mean that your organization or client is likely overpaying. REPEAT these steps once per month.
— Tip —
Tuesday Tip of the Week: If I were a plan sponsor here are the seven things I would be asking of PBMs during an RFP
RFP season is in full swing and a little later than usual for obvious reasons. It’s mind-boggling what PBMs are asked to do in some of these RFPs. The responses we provide are sophisticated. Isn’t it reasonable to then expect that the evaluation of those responses be equally sophisticated? If I were a plan sponsor here are the seven things I would be asking of PBMs during an RFP.
1. PBM Contract. Do you know why spreadsheeting PBM pricing offers is held in such high regard? Business math is easy 2 + 2 = 4. PBM contract evaluation isn’t so easy so decision-makers hand it off to the corporate attorney who can’t tell you the difference between ASP and WAC. I’m not suggesting the corporate attorney isn’t smart. Of course they are smart but that doesn’t mean diddly squat unless you have a trained-eye for pharmacy benefits. The problem for plan sponsors who wait until the last minute to address contract nomenclature is that it is the most important factor in determining whether your plan overpays or pays a fair price for PBM services. In PBM contracts 2 + 2 ≠ 4. Discount and rebate guarantees mean less when contract nomenclature is ambiguous.
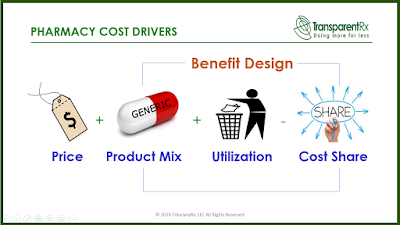
2. Benefit Design. Never once during hundreds of RFPs has any consultant or broker ever asked us for a completed benefit design as part of our response. I’ve not taken a poll so I don’t know the reason. Maybe it is because some believe benefit design doesn’t have a big role in determining cost. If that is the case, nothing could be further from the truth. Don’t put 50 questions in a RFP around benefit design where important details get lost in translation…geesh. I would be asking for a benefit design to be submitted as if we were going live with it. In pharmacy cost drivers, price is 1A and benefit design is 1B. Aside from copayments and deductibles (cost sharing) most plan sponsors know little else about their benefit design and have left it up to the PBM to decide. When the PBM is non-fiduciary that could lead to significant overpayments.
 |
| Click to Learn More |
3. References. 2-3 companies who can verify the PBM’s claims (i.e. retail network, mail and specialty access and transparency) about performance. This could also include inquiries about account management and member support performance.
4. Questionnaire. 20 – 25 verifiable questions pertinent to my company’s needs. Here is where you inquire about security, reporting, disease management, MTM or alternate funding programs.
5. PBM Reverse Auction. Two PBM reverse auctions in the same competitive bidding process in fact. The first round is conducted after the claims repricing is submitted. The second round is completed after all contract concessions have been made and the resulting contracts memorialized. Usually you are down to 3-5 candidates at this point. Keep in mind that in a well run and organized reverse auction prices only go down.
6. Finalist Presentation or Interview. Don’t allow PBMs to turn it into a marketing contest. Use the time to win more contract concessions and clear up any lingering concerns.
7. Claims Repricing. Not for the purpose of determing who has the better price but to make sure the PBM is in the ballpark of the market. Claims repricings tell you what happened in the past. Claims repricings can’t tell the story of what is going to happen in the future. The PBM contract and benefit design are better suited to help predict future performance. Furthermore, if the incumbent PBM has leveraged bad product mix or poor utilization to generate its management fee you are asking PBMs in the bidding process to reprice those same bad claims.
Now score each of the six areas (excluding repricing). Here are some weights I recommend applying to each score:
Contract – 40%
Benefit Design – 25%
References – 10%
Questionnaire – 5%
Reverse Auction – 15%
Finalist Presentation – 5%
As you can see the repricing has earned no weight. The claims repricing serves to show only if the pricing is competitive nothing more. The reverse auction will establish pricing guarantees and the contract will help determine whose pricing is the most transparent. It takes time to get really good at any of these areas. Don’t give up on them the first or even second time around.
The best proponent of radical transparency and lowest net Rx cost is informed and sophisticated purchasers of PBM services. I’m not talking about 1400 SAT or 4.0 GPA sophistication. I’m referring to a high level of sophistication in the PBM arena. If it isn’t your bag don’t carry it. Find someone else who specializes to do the heavy lifting for you.
Reference Pricing: “Gross” Invoice Cost vs. AWP for Popular Generic and Brand Prescription Drugs (Volume 325)
This document is updated weekly, but why is it important? Healthcare marketers are aggressively pursuing new revenue streams to augment lower reimbursements provided under PPACA. Prescription drugs, particularly specialty, are key drivers in the growth strategies of PBMs, TPAs, and MCOs pursuant to health care reform.

Step #4: Now take it one step further. Check what your organization has paid, for prescription drugs, against our acquisition costs then determine if a problem exists. When there is more than a 5% price differential for brand drugs or 25% (paid versus actual cost) for generic drugs we consider this a potential problem thus further investigation is warranted.
Multiple price differential discoveries mean that your organization or client is likely overpaying. REPEAT these steps once per month.
— Tip —
Always include a semi-annual market check in your PBM contract language. Market checks provide each payer the ability, during the contract, to determine if better pricing is available in the marketplace compared to what the client is currently receiving.
- Go to the previous page
- 1
- …
- 45
- 46
- 47
- 48
- 49
- 50
- 51
- …
- 140
- Go to the next page