Speakers at the 2017 annual meeting of the Academy of Managed Care Pharmacy took on rising health-care costs. In a presentation, Steven G. Avey, RPh, MS, FAMCP, Vice President of Specialty Clinical Programs and Michael Ciarametaro, MBA, Vice President of Research at the National Pharmaceutical Council, spoke on the issue and its effects on pharmacy.
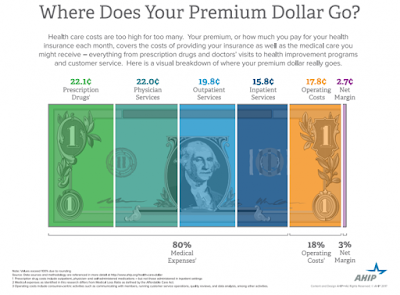
A major problem for patients and the health-care system—how higher-than-anticipated drug prices and patients who are stuck with more of the cost burden means more nonadherence and waste. For nonspecialty drugs, patient copays represent 20% to 25% of the drug’s cost, but for specialty drugs, copays represent less than 2% of the medication’s total cost. Avey was surprised, however, to see that financial concerns only represented 2% of patient responses in a patient survey.
The number one thing payers can do, Avey said, is to avoid waste, by addressing poor adherence, paying for the wrong dosage, gaps in care or inappropriate dosing, and prescribing drugs that are not indicated for the patient’s genetic mutation status. To prevent waste, he stressed that it is important for the specialty pharmacy to contact the provider and ask why a patient is not receiving or taking the appropriate regimen.
Ciarametaro discussed affordability, which is different for each stakeholder in the health-care system (patients, payers, society, or purchaser). He also made the distinction between affordability, value, and budget impact. “I would argue that increasing drug spending is not necessarily a negative indicator. We still need to figure out how much we should spend on drugs,” he said.
PBMs only have limited tools to deal with costs and interact with the various stakeholders, and they must deal with and balance covered therapies, utilization management, patient out-of-pocket costs, and rebate contracting with regard to premiums. A single determination of value is not adequate and needs to be tailored to the population, the condition, and the region of care, he said.
Read more >>