Implementing Reference Pricing Led to Changes in Drug Selection, Lower Spending
 |
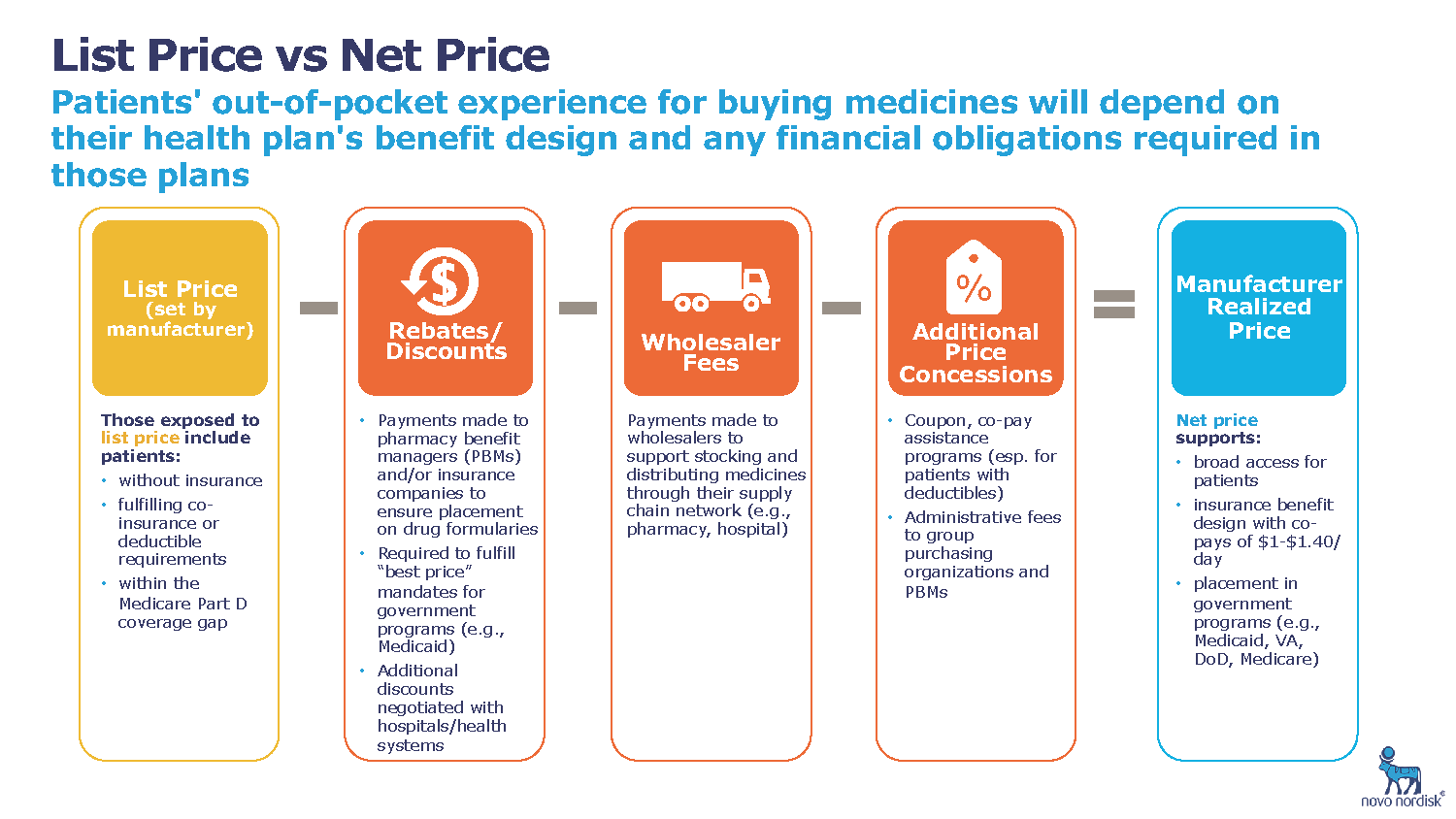
| FIGURE 1: Basic supply chain example from manufacturer to consumer |
A reference pricing initiative was linked to more prescription fills of lowest-priced drugs and a decreased average price per prescription, but higher rates of copayments by patients, a new study finds.
Reference pricing is a price control mechanism where an insurer or employer specifies the highest amount it will contribute towards paying for a drug or service, leaving patients to pay the additional cost if they choose an option priced higher than that benchmark. A recent study published in the New England Journal of Medicine examined the results of a reference pricing program implemented by the healthcare purchasing organization RETA Trust in 2013.
The program set the trust’s maximum drug payment for 1302 drugs in 78 classes at the price of the least expensive drug in each category. Unless an exemption was granted for clinical reasons, patients choosing a drug that was not the least costly would have to pay the difference in price.
Using pharmacy claims from 2010 to 2014, researchers analyzed changes in drug selection and expenditures after the implementation of reference pricing for the 17,500 employees covered by the RETA Trust. Members of a labor union which did not use reference pricing served as a comparison group to control for market trends.
Analyses indicated that more prescriptions were written for the lowest-priced drug in each therapeutic class for members of the RETA Trust after reference pricing was instituted. Specifically, the share of such prescriptions increased from 59.5% in July 2010 to 69.7% during the first quarter after reference pricing was implemented in July 2013. Over this time, the share of prescriptions written for the least costly drug among the labor union members did not change.
Tyrone’s comment: Reference pricing is a great first step. The article doesn’t mention it but I’m curious to know how the final cost [for the lowest priced drug in each category] to the labor union was determined. The point I’m making is even with an effective tool such as reference pricing to aid in price control there is still quite a bit of price uncertainty. AWP minus, AAC plus and WAC + all have different cost implications on both sides of the claim. I often play devils advocate so I’m happy to see the reference pricing strategy implemented with such a large organization. Assessing transparency will be more effectively done by a trained eye with personal knowledge of the purchaser’s benefit and disclosure goals. My hope is that the RETA Trust will continue to eliminate waste whilst not negatively impacting its members’ healthcare outcomes.
Researchers also determined that reference pricing had an effect on the RETA Trust’s expenditures. Before reference pricing, the trust paid around 10.6% more per prescription than the union, but after the change it paid prices that were 13.9% lower than those paid by the union, equivalent to a $9.24 lower average price per monthly prescription. Extrapolated to the total number of prescriptions filled in the 18 months after implementation, the RETA Trust saved $1.34 million in this time.