Tuesday Tip of the Week: PBMs are Under Attack But Commercial Employers Get Little Help
On the heals of SCOTUS’s recent ruling, several states have passed legislation to regulate PBMs. The United States Supreme Court declared in Rutledge v. Pharmaceutical Care Management Association that states do have the ability to pass legislation that requires pharmacy benefit managers to reimburse pharmacies for drugs at a rate equal to or higher than the pharmacies’ wholesale cost.
In its unanimous 8-0 opinion, the Court ruled that Arkansas’s law is not preempted under ERISA and that states may enact laws that regulate PBM reimbursement costs to pharmacies. Now, there is a model law making its way through the National Association of Insurance Commissioners (NAIC) that would establish a licensure requirement and rules of conduct for PBMs.
(2) Prohibition on Gag Clauses – A PBM may not prohibit a pharmacist from (i) discussing information regarding the total cost for pharmacist services for a prescription drug.
(3) Limitation on Price – A PBM may not require a covered person purchasing a covered prescription drug to pay an amount greater than the lesser of (i) the covered person’s cost-sharing amount and (ii) the amount the covered person would pay for the drug if the covered person were paying the cash price.
There is little doubt that the Supreme Court’s ruling is going to cut into non-fiduciary PBMs’ cash flow. They are going to be required to reimburse pharmacies more and will no longer be able to charge the higher copay when the ingredient cost is lower (clawback), for example. Yet, non-fiduciary PBM revenues and profits will continue to grow but how? They will shift the cost but where? Unsophisticated commercial employers will undoubtedly pick up the lion’s share of the cost shift.
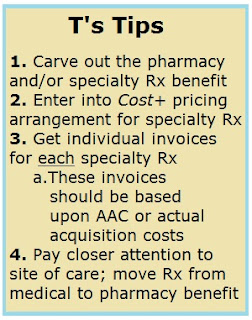
In 2020, specialty drug spending outweighed traditional drug spending for the first time ever. Commercial employers must engage all stakeholders and develop a pharmacy benefits management strategy which centers around high-cost ($15,000 or more per year) drug therapies. It goes without saying, any effort by a non-fiduciary PBM to protect its profit margins will start and end with specialty drugs.