Drug companies favor biotech meds over pills, citing new U.S. law [Weekly Roundup]
Drug companies favor biotech meds over pills, citing new U.S. law other notes from around the interweb:
- Drug companies favor biotech meds over pills, citing new U.S. law. Drugmakers are prioritizing complex biotech medicines over treatments that can be given as pills because recent U.S. legislation gives biologics a longer runway before becoming subject to government price limits, top industry executives said this week. The Inflation Reduction Act (IRA), which Democrats passed last August, for the first time allows the government’s Medicare health plan for people aged sixty-five and over to negotiate the prices it is willing to pay for certain medications. The law sets a nine-year exemption period for “small molecule” drugs, which are mainly pills, while “large molecule” biologics, generally injections or infusions, are protected from negotiation for 13 years. “The difference between a nine- and 13-year product line is about 50 or 60% of the value,” Eli Lilly Chief Executive Officer Dave Ricks said in an interview. “In 10 years, we’ll have far fewer small molecules being developed than we do today.”
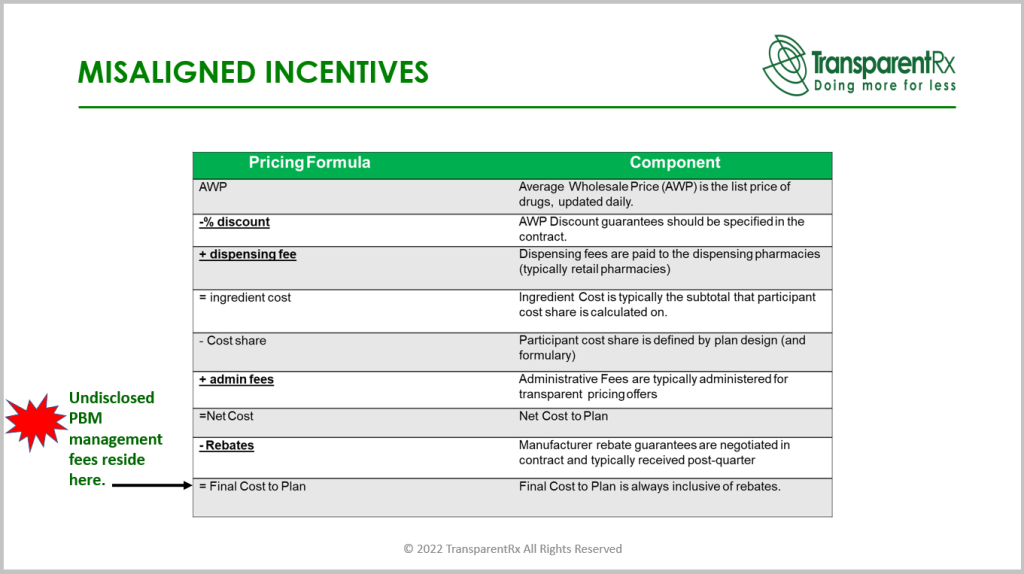
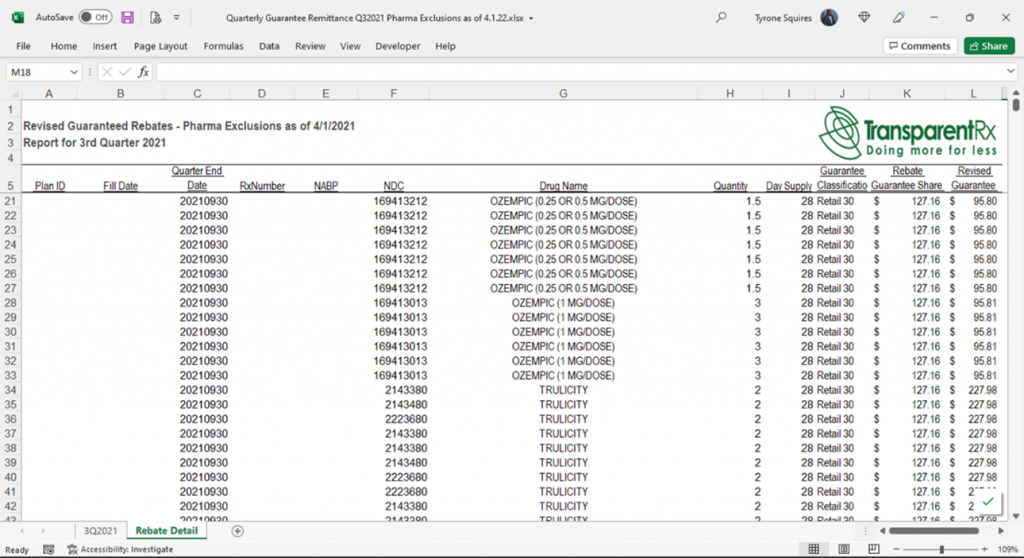
- FTC action on PBMs could be just what the doctor ordered to improve patient outcomes. The stated purpose of PBMs is to alleviate some of the administrative burden related to processing prescription drug claims and optimizing drug utilization to help manage costs for plan sponsors. Unfortunately, most PBMs have evolved to become vertically integrated pharmacies and adopt opaque business practices that mostly benefit only themselves. For example, pharmaceutical rebates have become a cash cow for PBMs. Paid out by drug manufacturers, these rebates are designed to help lower the price burden of new drugs by reimbursing plan sponsors a portion of the cost each time they’re filled at the pharmacy. The problem is, PBMs are under no obligation to pay the full rebate back to the plan sponsor, and many PBMs pocket a substantial portion, if not all, of these rebates, often with plan sponsors completely unaware.

- California sues largest US insulin manufacturers and PBMs for overpricing. Eli Lilly, Novo Nordisk, and Sanofi produce over 90% of the global insulin supply and the PBMs CVS Caremark, Express Scripts and OptumRx administer pharmacy benefits for around 80% of prescription claims managed. The lawsuit, filed in the California Superior Court in Los Angeles, argues that because competition is highly limited in both their markets, these six companies can keep ‘aggressively hiking’ the list price of insulin at the expense of patients, violating the state’s Unfair Competition Law. According to a 2021 Congressional report, Eli Lilly, Novo Nordisk, and Sanofi have raised the price of their insulin by 1,219%, 627% and 715%, respectively, since they were first launched.
- How Coupons Keep Drugs Costly. An economist who holds a joint appointment at the Harvard Kennedy School, began studying this topic more than a decade ago, prompted by the growing number of pharmaceutical ads that included coupons. Such coupons offer consumers a discount on the co-pay for the advertised drug and have grown increasingly popular; the share of brand-name prescription drug spending that included a coupon rose from 26 percent in 2007 to 90 percent in 2017, Leemore S. Dafny reports. And the number of drugs with available coupons rose from about 200 in 2008 to more than 800 in 2018. Not everyone is eligible for coupons; Medicare enrollees are prohibited by law from using them. “The coupons are considered kickbacks or financial inducements to consume a product that is reimbursed by the federal government,” Dafny explains, and are therefore banned in that context. But pharmaceutical companies are permitted to donate to independent charities that subsidize co-pay assistance for patients, even those on Medicare, and to earmark those donations for conditions treated by drugs they make.