Report: “Specialty” drugs are by far the most expensive, but classification seems arbitrary [Weekly Roundup]
Report: Specialty drugs are by far the most expensive, but classification seems arbitrary and other notes from around the interweb:
- Report: “Specialty” drugs are by far the most expensive, but classification seems arbitrary. The prescriptions with the most astonishing price tags — like cancer meds that can cost more than $20,000 a month — are usually classified as “specialty” drugs. You’d think that since they’re so costly, there would be clear criteria for putting drugs in the specialty category. But, according to a new report, you’d be wrong. The issue might seem arcane, but it’s hugely important. Specialty drugs account for only about 2% of the volume of drugs dispensed in the United States, according toq industry estimates, but they also account for more than 50% of overall drug spending. The report, by data analysis firm 46Brooklyn Research, found that the three largest drug middlemen in the United States often don’t classify the same medicines as specialty. It also said that a substantial portion of the ones they do put into that category are generics — drugs that are usually no longer under patent and thus are supposed to be cheaper because multiple drugmakers can supply them.

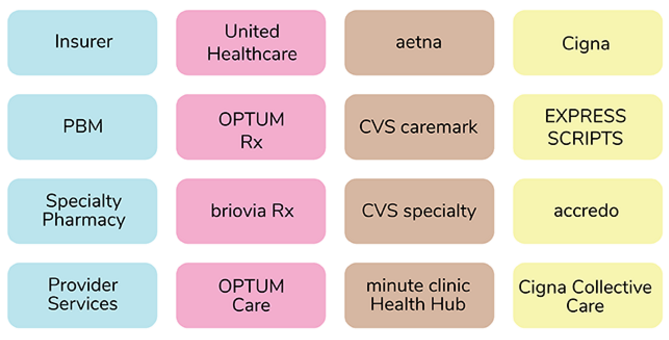
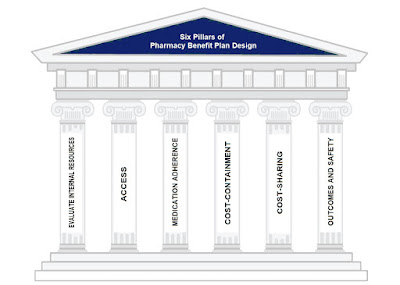
- How Payers Can Cut Through the Noise and Optimize Their PBM Partnerships. Some payers and PBMs are owned by the same parent companies, and in fact, they make up a large share of the market — something that has attracted scrutiny. The complicated relationships between these large, combined entities make it important to build a working partnership that aligns with the goals of cost-effective, high quality and accessible care. As payers work to optimize their PBM partnerships, the complexity of their agreements makes it important to increase understanding and apply best practices to ensure transparency and value. The thought of switching PBMs can be overwhelming and often immobilizes payers instead of evaluating opportunities that would drive a more sustainable sound partnership. Payers need PBMs as partners to provide core critical functions. To optimize their relationship, payers can take several key steps.
- What employers want to see as Congress aims to reform PBMs. A key Senate committee last week advanced a bill that includes several significant reforms to pharmacy benefit managers, including a ban on spread pricing. However, one provision that was left on the cutting room floor is a change that many employers are still hopeful to see, Alan Gilbert, vice president of policy at the Purchaser Business Group on Health (PBGH), told Fierce Healthcare. And that’s establishing PBMs as fiduciaries. While the Senate Health, Education, Labor, Pensions (HELP) committee considered a similar policy change, what made the final cut was instead a directive to the Department of Labor to study the issue to enable legislation in the future. Gilbert said that making PBMs fiduciaries in the pharmacy benefits process would hold them as accountable as health plans and plan sponsors. Pushing these companies to have more skin in the game would be key to curbing the worst of their behavior, he said.
- The Price of the PBM. One crucial element of the US drug supply chain is the wholesaler, who purchases drugs from manufacturers using purchasing power to gain discounts that average around 16 percent, according to IQVIA data. About 92 percent of prescription drugs are distributed through the three largest pharmaceutical wholesalers, McKesson, AmerisourceBergen, and Cardinal. Wholesalers earn revenue through “forward-buying,” purchasing extra inventory at current prices to sell them in future at a revised higher price.