The Definition of Oversee: to watch over and direct (an undertaking, a group of workers, etc.) in order to ensure a satisfactory outcome or performance.
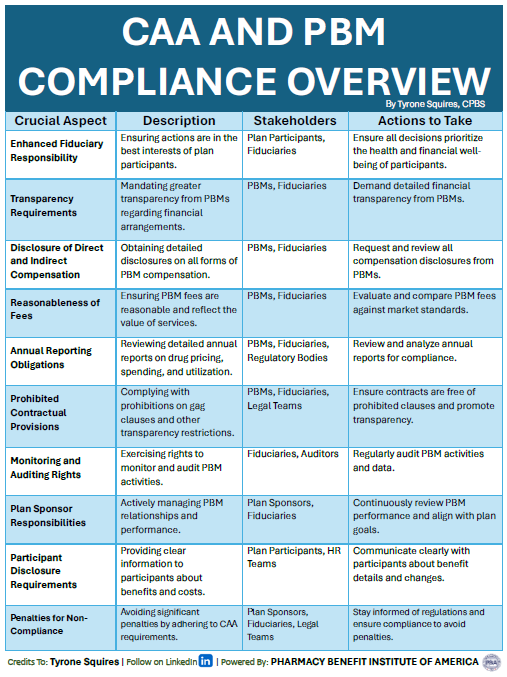
As a CHRO, it’s crucial to stay informed about the impact of the CAA on your fiduciary responsibilities in managing pharmacy benefits. Here are ten key aspects in understanding the Consolidated Appropriations Act (CAA) for pharmacy benefit management:
Enhanced Fiduciary Responsibility: Prioritize the best interests of plan participants.
Transparency Requirements: Demand greater financial transparency from PBMs.
Disclosure of Direct and Indirect Compensation: Obtain detailed disclosures on all PBM compensation.
Reasonableness of Fees: Ensure PBM fees are reasonable and reflect service value.
Annual Reporting Obligations: Review detailed annual reports on drug pricing and utilization.
Prohibited Contractual Provisions: Comply with prohibitions on gag clauses and other restrictions.
Monitoring and Auditing Rights: Regularly audit PBM activities and data.
Plan Sponsor Responsibilities: Actively manage PBM relationships and performance.
Participant Disclosure Requirements: Provide clear information to participants about benefits and costs.
Penalties for Non-Compliance: Avoid penalties by adhering to CAA requirements.
? Continuous Learning is Key ?
Engage in ongoing education and training to stay updated on regulatory changes and industry best practices. This will ensure you are well-equipped to navigate the complexities of the CAA and maintain compliance, ultimately protecting the interests of your plan participants and organization. Understanding the Consolidated Appropriations Act (CAA) for pharmacy benefit management is a key aspect of plan fiduciary responsibility.
Health plan sponsors must manage plan assets wisely and solely for the benefit of participants and beneficiaries. Fiduciaries are expected to possess expertise in their field or to seek guidance from subject-matter experts. The standard they must meet is that of a prudent expert, not just a well-intentioned layperson. Merely making a good faith effort does not suffice.
The video “Unlocking the Secrets of PBMs: Strategies to Navigate Their Profit Tactics” is an insightful 59-minute presentation designed to equip employers and benefits consultants with the necessary tools to effectively manage and negotiate with pharmacy benefit managers (PBMs). Over the course of the video, viewers are introduced to the various profit-making tactics employed by PBMs and the impact these can have on pharmacy costs and patient outcomes. Mastering PBM negotiations is an essential tool for CHROs, CFOs, and benefits consultants.
Key sections of the video delve into understanding the opaque pricing models that PBMs often use, which can obscure actual drug costs and complicate efforts to ensure fair pricing. The video provides practical strategies to unveil these hidden costs and leverage this transparency in negotiations. It also discusses the importance of contract clarity and how to ensure contracts are devoid of loopholes that could increase costs unexpectedly.
Furthermore, the video highlights the significance of staying informed about industry trends and regulatory changes that can affect PBM contracts. It advises on building a collaborative relationship with PBMs while maintaining a vigilant stance that prioritizes fiduciary responsibilities. For employers and benefits consultants, this video is an essential tool, offering actionable advice on how to reduce pharmacy costs without compromising on the quality of patient care.
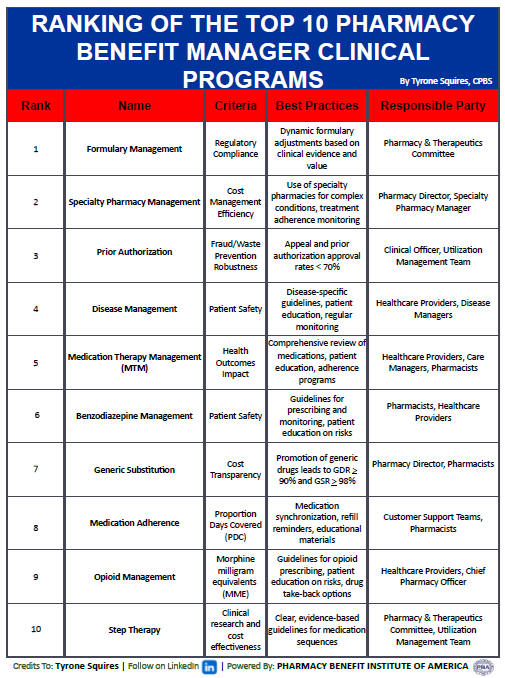
This document presents a detailed evaluation of the top 10 clinical programs offered by pharmacy benefit managers (PBMs), which are pivotal for optimizing drug management and enhancing patient care while maintaining cost-effectiveness. The evaluation of top 10 pharmacy benefit manager clinical programs is methodically ranked, each program focusing on various aspects of clinical pharmacy benefit management.
Formulary Management: Topped by dynamic formulary adjustments, this program ensures regulatory compliance and the integration of clinical evidence to drive value-based decisions.
Specialty Pharmacy Management: This handles complex conditions through specialty pharmacies, emphasizing treatment adherence and efficiency.
Prior Authorization: Focused on fraud and waste prevention, this program maintains robust prior authorization processes with an approval rate below 70%.
Disease Management: Offers disease-specific guidelines and regular patient monitoring to enhance patient safety and health outcomes.
Medication Therapy Management (MTM): A comprehensive review of patient medications is combined with education and adherence programs to improve health impacts.
Benzodiazepine Management: This focuses on safe prescribing practices and patient education regarding the risks associated with benzodiazepines.
Generic Substitution: Promotes the use of generic drugs to enhance cost transparency and increase generic dispensing rates.
Medication Adherence: Utilizes medication synchronization and refill reminders to improve the proportion of days covered.
Opioid Management: Enforces guidelines on opioid prescribing, patient education on risks, and drug take-back options to manage opioid use effectively.
Step Therapy: Implements clear, evidence-based guidelines for medication sequences to ensure clinical and cost-effectiveness.
Each program is backed by best practices and involves key stakeholders like Pharmacy Directors, Healthcare Providers, and Pharmacy & Therapeutics Committees, ensuring a holistic approach to pharmacy benefits management. This ranking is crafted to assist Chief Human Resources Officers (CHROs) and Chief Financial Officers (CFOs) in making informed decisions about which clinical programs can best meet their organizational needs, align with financial goals, and ensure patient safety and satisfaction.
New Lawsuit Targets Opioid Pharmacy Benefit Managers. The case is before federal Judge Dan Aaron Polster of the United States District Court for Northern Ohio based in Cleveland. “Judge Polster recently opened a new bellwether track of cases against Express Scripts and OptumRx, two of the three PBMs with the largest market share in the United States,” according to the National Opioid Litigation letter. The other company in that top three is CVS Caremark, a subsidiary of CVS Health, that was included in a recent $10 billion settlement that also involved Walgreens…”About those companies, Marcus told the commissioners, “They chose profits over doing the right thing.”
Fiduciary Duty Update: PBM Audit is Now Mandatory Protocol. The revelation that a drug costing over $10,000 in the market could be sourced for $28.40 has sent shockwaves through the industry, illustrating a glaring oversight in PBM management. Auditing your PBM is not merely a best practice; it is a critical safeguard against financial inefficiency and legal liabilities. Audits reveal discrepancies in billing, conflicts of interest, and non-compliance with contract terms — issues that, if unaddressed, could lead to breach of fiduciary claims.
Audit of the American Postal Worker’s Union Health Plan’s Pharmacy Operations. “We found that the PBM overcharged the Carrier and the FEHBP $44,882,688 (including lost investment income) by not passing through all discounts and credit related to prescription drug pricing that were required under the PBM Transparency Standards found in the Carrier’s contract with the OPM. Specifically, our audit identified the following six findings that require corrective action. The findings occurred across all years of the auto scope unless otherwise noted.”
Why Are Cash Prices Lower Than Health Insurance Negotiated Prices? Growing evidence demonstrates a counterintuitive phenomenon in healthcare: the cash price is often cheaper than insurance prices for the same service or product. Cash prices are unilaterally determined by a provider, while insurance prices are bilaterally negotiated between a provider and an insurance company. Don’t insurance companies presumably possess more bargaining power than individual patients? Our study found that among common shoppable services—such as lab tests, imaging, and joint replacements—half of U.S. hospitals set cash prices lower than their median insurance negotiated prices. Cash price being cheaper than insurance prices has also been documented for prescription drugs.
In the modern healthcare landscape, the Pharmacy Benefits Manager (PBM) industry stands as a pivotal intermediary between patients, healthcare providers, and pharmaceutical companies. PBMs play a crucial role in managing prescription drug benefits for health insurance plans, ensuring cost-effective access to medications for millions of individuals. However, behind the scenes of this complex ecosystem lies a fundamental pillar driving efficiency, innovation, and seamless operations—the Information Technology (IT) department.
The convergence of healthcare and technology has transformed the way PBMs operate, and the IT department serves as the engine powering this transformation. From streamlining processes to safeguarding sensitive data, the IT team within a PBM organization plays a multifaceted role that directly impacts the quality of care delivered to patients and the effectiveness of prescription drug benefit management.
1. Infrastructure and Systems Management
At the core of every PBM’s operations lies a robust infrastructure comprising databases, networks, and software systems. The IT department is responsible for designing, implementing, and maintaining this infrastructure to ensure seamless connectivity and data accessibility across various stakeholders. From electronic health records (EHR) integration to claims processing platforms, IT professionals deploy and manage the technological backbone that supports the entire PBM ecosystem.
2. Technical Implementations with Third-Party Administrators
Within the Pharmacy Benefits Manager (PBM) industry, the Information Technology (IT) department plays a crucial role in managing technical implementations with third-party administrators (TPAs). This entails overseeing the integration of systems, data exchange protocols, and ensuring seamless connectivity between the PBM’s infrastructure and the systems utilized by TPAs. The IT team collaborates closely with TPAs to configure interfaces, establish secure connections, and troubleshoot any technical issues that may arise during the implementation process. By leveraging their expertise in software integration, network architecture, and data management, the IT department ensures that the partnership between the PBM and TPAs operates smoothly, facilitating efficient prescription drug benefit management and enhancing the overall customer experience.
3. Data Analytics and Business Intelligence
In an industry driven by data, PBMs rely on sophisticated analytics to identify trends, manage costs, and optimize patient outcomes. The IT department plays a pivotal role in developing and maintaining data analytics platforms that sift through vast amounts of information to provide actionable insights. By leveraging technologies such as artificial intelligence and predictive analytics, IT teams help PBMs make informed decisions regarding formulary management, medication adherence programs, and provider network optimization.
4. Security and Compliance
With the increasing digitization of healthcare data, ensuring the security and privacy of sensitive information is paramount. The IT department within a PBM organization is tasked with implementing robust cybersecurity measures to safeguard patient data from unauthorized access, breaches, and cyber threats. Moreover, IT professionals work closely with regulatory bodies to ensure compliance with stringent healthcare regulations such as the Health Insurance Portability and Accountability Act (HIPAA).
5. Digital Health Innovation
As healthcare continues to embrace digital transformation, PBMs are leveraging innovative technologies to enhance patient engagement and medication management. The IT department works to develop and deploy digital health solutions such as mobile applications, electronic Prior Authorization platforms, etc. These technologies not only empower patients to take control of their health but also facilitate real-time communication between healthcare providers, pharmacists, and insurance companies.
6. Customer Experience Enhancement
In an era where customer experience reigns supreme, PBMs are leveraging technology to streamline processes and enhance service delivery. The IT department plays a critical role in developing user-friendly portals, automated communication systems, and interactive tools that empower patients to navigate their prescription drug benefits with ease. By prioritizing usability and accessibility, IT professionals contribute to improving patient satisfaction and loyalty while driving operational efficiency within the PBM organization.
7. Collaboration and Integration
Effective communication and collaboration are essential for the seamless coordination of care within the healthcare ecosystem. The IT department acts as a catalyst for integration, facilitating interoperability between disparate systems used by pharmacies, healthcare providers, and insurance companies. IT professionals enable the seamless exchange of patient information, prescriptions, and clinical data across different stakeholders.
Conclusion
In the Pharmacy Benefits Manager industry, the role of the Information Technology department cannot be overstated. From infrastructure management to data analytics, cybersecurity, and digital innovation, IT professionals play a pivotal role in driving efficiency, enhancing patient care, and ensuring compliance within PBM organizations. As healthcare continues to evolve, the collaboration between IT and healthcare professionals will be instrumental in shaping the future of prescription drug benefit management and improving health outcomes for individuals worldwide.
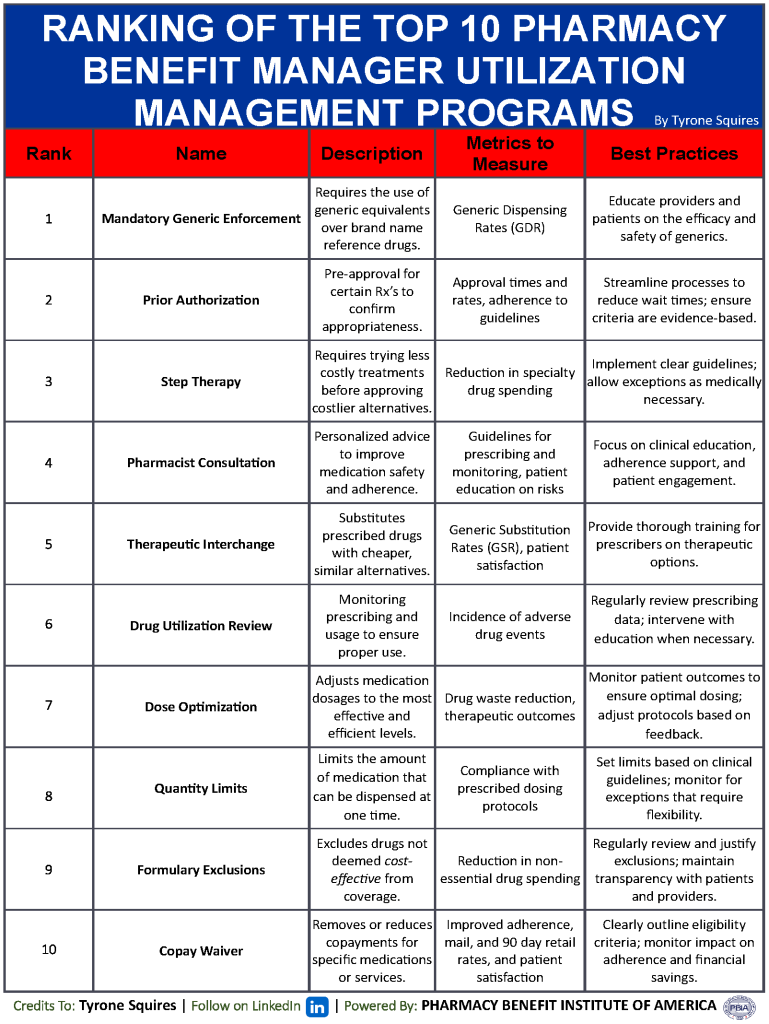
Ranking the top utilization management (UM) programs used by Pharmacy Benefit Managers (PBMs) can be complex due to the proprietary nature of specific tools and strategies employed by different organizations. However, several key types of UM programs are commonly recognized as effective in managing pharmacy benefits and controlling costs while ensuring patient care. Here’sTransparentRx’s ranking of the top ten pharmacy benefit manager utilization management programs:
Pharmacy benefits must be carefully managed to ensure people receive cost-effective treatment, improving their well-being and helping them lead happier, longer lives. This also enables employers to maintain a healthy and engaged workforce. These UM programs form the core of what many top PBMs use to manage drug utilization effectively. Each program has its strengths and plays a critical role in balancing cost containment with the provision of high-quality care. The specific effectiveness and ranking can vary depending on the specific health populations managed and the overall strategy of the PBM.
Audit of the American Postal Worker’s Union Health Plan’s Pharmacy Operations. “We found that the PBM overcharged the Carrier and the FEHBP $44,882,688 (including lost investment income) by not passing through all discounts and credit related to prescription drug pricing that were required under the PBM Transparency Standards found in the Carrier’s contract with the OPM. Specifically, our audit identified the following six findings that require corrective action. The findings occurred across all years of the auto scope unless otherwise noted.”
Why Are Cash Prices Lower Than Health Insurance Negotiated Prices? Growing evidence demonstrates a counterintuitive phenomenon in healthcare: the cash price is often cheaper than insurance prices for the same service or product. Cash prices are unilaterally determined by a provider, while insurance prices are bilaterally negotiated between a provider and an insurance company. Don’t insurance companies presumably possess more bargaining power than individual patients? Our study found that among common shoppable services—such as lab tests, imaging, and joint replacements—half of U.S. hospitals set cash prices lower than their median insurance negotiated prices. Cash price being cheaper than insurance prices has also been documented for prescription drugs.
Fiduciary Duty Update: PBM Audit is Now Mandatory Protocol. The revelation that a drug costing over $10,000 in the market could be sourced for $28.40 has sent shockwaves through the industry, illustrating a glaring oversight in PBM management. Auditing your PBM is not merely a best practice; it is a critical safeguard against financial inefficiency and legal liabilities. Audits reveal discrepancies in billing, conflicts of interest, and non-compliance with contract terms — issues that, if unaddressed, could lead to breach of fiduciary claims.
How GoodRx Helped Steal $7 From My Pharmacy. GoodRx, primarily known as a platform for obtaining prescription coupons and tracking drug prices, interacts with Pharmacy Benefits Managers (PBMs) in a way that’s distinct from traditional PBM operations. In essence, GoodRx leverages the existing PBM infrastructure to provide discounted prices directly to consumers, often bypassing the more traditional insurance-based prescription purchasing pathway. For benefits consultants and employers, understanding this interaction is crucial in advising on healthcare strategies that maximize both cost efficiency and patient outcomes. Employers need to consider how tools like GoodRx fit into a broader benefits design, particularly in terms of how they affect out-of-pocket costs for employees and the overall usage of pharmacy benefits managed under traditional PBM contracts.
In our webinar, “Revolutionizing Pharmacy Benefits by Disrupting the Status Quo and Driving Down Costs,” we delve into the innovative strategies reshaping the landscape of pharmacy benefits management (PBM). By challenging conventional approaches and implementing cutting-edge solutions, we’re driving down costs while enhancing patient outcomes.
Why You Should Watch:
Gain Insight: Learn about groundbreaking methodologies transforming pharmacy benefits, equipping you with the knowledge to navigate this evolving industry.
Cost Reduction Strategies: Discover practical approaches to reducing pharmacy costs without compromising the quality of care, crucial for businesses seeking to optimize their healthcare spending.
Patient-Centric Solutions: Explore how our innovative techniques prioritize patient well-being, ensuring better health outcomes while containing expenses.
Industry Disruption: Stay ahead of the curve by understanding the latest disruptions in the PBM sector and how they can benefit your organization.
Fiduciary Standard of Care: Understand the importance of adopting a fiduciary standard of care in pharmacy benefits management, aligning with best practices and ethical standards.
Stand Out Among Your Peers
Who Should Watch:
Benefits Consultants: Enhance your expertise in PBM to better serve your clients and provide them with actionable strategies to control healthcare costs.
Human Resources Managers: Gain insights into innovative approaches for managing pharmacy benefits, helping you make informed decisions that benefit your employees and your bottom line.
Healthcare Professionals: Stay abreast of industry trends and advancements in pharmacy benefits management, enabling you to deliver more effective patient care within your organization.
Watch on-demand as we revolutionize pharmacy benefits together, driving down costs while prioritizing patient well-being. Let’s disrupt the status quo and shape the future of healthcare together!
In today’s rapidly evolving healthcare landscape, managing pharmacy benefits is not just about containing costs—it’s about crafting a synergy of quality care, accessibility, efficiency, and participant satisfaction. At TransparentRx, we understand that every aspect of pharmacy benefit design can significantly impact the health and well-being of the participants it serves. Let’s delve into the four broad issues that underpin an effective pharmacy benefit design.
1. Quality: The Pillar of Care
Quality in pharmacy benefits is threefold: care structure, processes, and outcomes. A robust care structure is foundational, ensuring that participants have access to essential medications without unnecessary delays or hurdles. The process, from prescription to pill delivery, must be streamlined, clear, and consistently monitored for potential improvements.
Outcomes are the ultimate measure of quality. At TransparentRx, we prioritize the clinical effectiveness of the medications provided and the positive health outcomes for the participant. This includes not only the resolution of the condition being treated but also monitoring for potential drug abuse, interactions, and side effects.
2. Accessibility: Removing Barriers
Accessibility goes beyond the physical availability of medications. It encompasses the elimination of financial, transportation, and geographical barriers that participants may face. TransparentRx champions affordable options without sacrificing quality. Whether it’s negotiating better prices or embracing mail-order services, we ensure that medications are within reach, both geographically and financially.
Transportation and geographical challenges are addressed by a network of pharmacies and the use of innovative delivery methods. By enhancing our telehealth and mail-order services, we bring the pharmacy to the participant’s doorstep, no matter where they live.
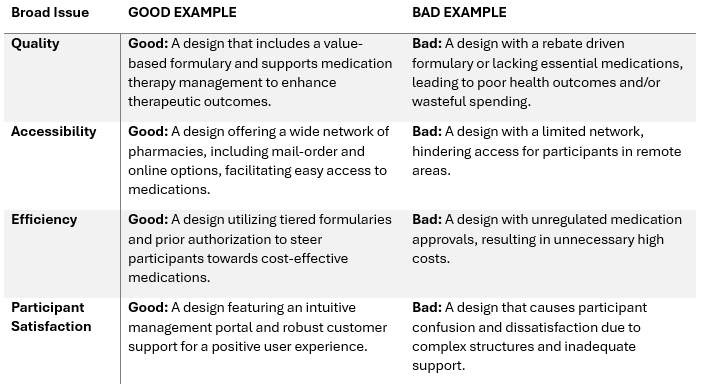
Understanding the distinctions between effective and ineffective benefit design practices is crucial. Below, we present a table contrasting strong (good) examples of benefit design with practices that should be avoided (bad) for each of the four broad issues:
By recognizing the stark contrast between these examples, employers, brokers, and consultants can more effectively evaluate and select pharmacy benefit plans that align with the fiduciary standard of care and participant-centric values. TransparentRx stands ready to guide you through the intricacies of these issues, ensuring that your pharmacy benefit design is both cost-effective and highly beneficial to your participants.
3. Efficiency: Maximizing Resources
Efficiency in pharmacy benefit design means accomplishing plan objectives with the least expensive combination of resources—without compromising on quality. At TransparentRx, we leverage InsourceRx data analytics to understand usage patterns, eliminate waste, and prevent fraud.
We assess the therapeutic equivalents and generic options, ensuring the most cost-effective medications are available. By balancing the cost against clinical effectiveness, we provide a plan that respects both the participant’s health and the bottom line.
4. Participant Satisfaction: The Heart of Our Mission
The true measure of a successful pharmacy benefit design is participant satisfaction. It reflects the ease of using the plan, the quality of the interactions with pharmacy staff, and the clarity of information provided. TransparentRx takes pride in our Net Promoter Score (NPS) of 86, which is a testament to our commitment to participant satisfaction.
This score significantly surpasses the industry average NPS for pharmacy benefit managers, reflecting the exceptional experience participants have with our services. An NPS of 86 indicates that a vast majority of our clients are not just satisfied, but are enthusiastic advocates for our brand, confident in recommending our services to others.
Conclusion
Pharmacy benefits management is a complex, multifaceted endeavor. By focusing on quality, accessibility, efficiency, and participant satisfaction, TransparentRx crafts a pharmacy benefits plan that not only meets but exceeds expectations. Our commitment to a fiduciary standard of care ensures that every decision we make is in the best interest of the participants we serve—helping our nation look better, feel better, and live longer.
Reviewing PBM Alternative Pricing Models For CVS Health, ESI, and OptumRx. PBM alternative pricing models are being rolled out by some of the biggest organizations in the industry in response to mounting political pressure, changing legislation, and the prevalence of industry disruptors. PSG has closely assessed the strategies put forward by CVS Health, ESI, and OptumRx regarding pharmacy reimbursement and client pricing models. We will take a deeper look at network contracting strategies like CVS CostVantage and ESI ClearNetwork in addition to client pricing strategies such as CVS Caremark TrueCost, ESI ClearCareRx, OptumRx Cost Advantage, and OptumRx Cost Clarity and share some considerations for how plan sponsors should address the changing pricing landscape.
GLPs Are the Latest Example of the Shift to Alternative Purchasing Models. Prior to the rollout of Medicare Part D in 2006, the Medicare population represented the largest out-of-pocket consumer group in the cash pay marketplace. Then it was the uninsured prior to the Affordable Care Act (ACA). Then, after the ACA exchanges and Medicaid expansion, the cash pay strategy turned to middle- and upper middle–class households, with the fewest regulatory restrictions, the most disposable income, and, importantly, the highest deductibles for drug coverage. Many of these individuals had to spend many thousands of dollars for first dollar coverage. A large swath of the American population has now become accustomed to not even bothering with their pharmacy benefit manager (PBM), and the first question that comes to mind isn’t “Does my insurance cover it?” but rather, “What’s the easiest and most convenient way for me to get a prescription for the drug I saw on my social media feed?”
Explainer: Why are US pharmacy benefit managers under fire? Separate bills aim to ban what is known as “spread pricing,” a practice in which PBMs charge health plans a larger amount for a drug than they pay out to pharmacies. Some are seeking more transparency under which the companies would be required to provide more information on their non-public negotiations. Rebates have also been a subject of proposed new government rules. The Trump administration sought in 2020 to make rebates illegal for Medicare prescription drug plans by removing the safe harbor protection that shields rebates from federal anti-kickback laws. The Biden administration delayed the rule until 2023 and Congress further delayed it until 2027.
How GoodRx Helped Steal $7 From My Pharmacy. GoodRx, primarily known as a platform for obtaining prescription coupons and tracking drug prices, interacts with Pharmacy Benefits Managers (PBMs) in a way that’s distinct from traditional PBM operations. In essence, GoodRx leverages the existing PBM infrastructure to provide discounted prices directly to consumers, often bypassing the more traditional insurance-based prescription purchasing pathway. For benefits consultants and employers, understanding this interaction is crucial in advising on healthcare strategies that maximize both cost efficiency and patient outcomes. Employers need to consider how tools like GoodRx fit into a broader benefits design, particularly in terms of how they affect out-of-pocket costs for employees and the overall usage of pharmacy benefits managed under traditional PBM contracts.
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.