The Definition of Oversee: to watch over and direct (an undertaking, a group of workers, etc.) in order to ensure a satisfactory outcome or performance.
Two paths. One decision. Understanding the difference shapes the outcome.
At a glance, the two paths can look almost identical. Both promise to manage prescription drug benefits, both use familiar language, and both claim to act in the plan’s best interest. But the direction they take a plan can differ in meaningful ways. Understanding the difference between a pharmacy benefit administrator and a pharmacy benefit manager is what determines clarity, control, and long-term outcomes for employers.
Since PBMs emerged decades ago to help plans manage prescriptions, rebates and discounts, they evolved into powerful intermediaries that influence almost every aspect of the drug benefit. They decide which drugs are covered, which pharmacies get paid, how much members pay, and how much the plan ultimately spends. The level of control is significant and often misunderstood.
Given the consolidation and vertical integration in today’s PBM market, it is important for plan sponsors and consultants to understand the difference between a PBA and a PBM. The decision comes down to what the plan actually wants: clean administration or full benefit management.
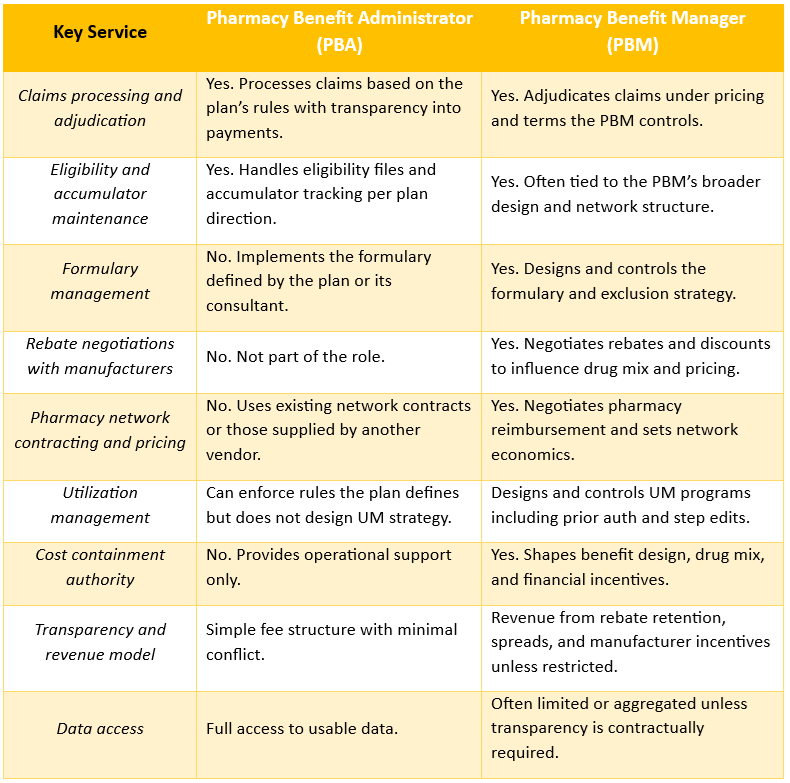
Here is a clear comparison of what each brings to the table.
A clear side-by-side view of how a pharmacy benefit administrator operates compared to a traditional PBM showing where control, incentives, and conflicts diverge for employers.
For many employers, brokers, and consultants, the distinction matters because it influences fiduciary risk, cost control, and member trust. A PBA offers clean operational execution with straightforward fees. A PBM offers full control over the drug benefit but can carry financial incentives that often run counter to the interests of the plan.
My take is simple. When cost, transparency, and accountability matter, a PBA or a fiduciary PBM model should be the starting point. If a PBM is used, the contract must eliminate hidden revenue, force full data access, and require meaningful audit rights. Without that structure, the plan will always choose the wrong path.
Author Bio
Tyrone Squires is Founder and Managing Director of TransparentRx, the first pharmacy benefit manager to operate under a true fiduciary standard of care. He trains benefit leaders across the country to manage pharmacy benefits in a way that delivers the outcomes their plans actually need. If you want help assessing where your plan stands, book a discovery call.
Every missed dose has a price: confusion today, complications and higher costs tomorrow.
Medication adherence determines whether a therapy delivers any value. In chronic disease, roughly half of all patients do not take their medications as prescribed. High out-of-pocket costs, poor care coordination, and unnecessary hurdles all contribute to missed fills or long gaps in therapy.
Employers feel the financial impact. Nonadherence drives avoidable hospitalizations, emergency room visits, and complications that spill into the medical plan. Lost productivity adds another layer of expense when conditions flare up because medications aren’t taken consistently. When prescriptions go unfilled, the employer pays for a benefit that never produces the expected clinical or financial return. (1)
This is why affordability matters. When members skip medications due to cost, adherence falls and overall costs rise. A PBM operating under a fiduciary standard has a duty to remove barriers, track adherence, and intervene early. Most PBMs do not. They track dispensing, not outcomes, and employers end up carrying the downstream burden. (2)
How Adherence Is Measured: MPR and PDC
Because it’s impractical to observe directly whether every patient takes every pill, the industry relies on proxy metrics using refill/claims data. Two widely accepted measures are:
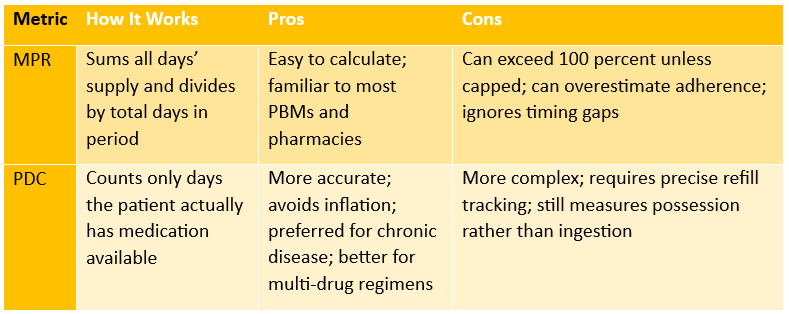
Medication Possession Ratio (MPR)
MPR = (total days’ supply dispensed over a given period) ÷ (number of days in that period) (3)
Example: If over a 365-day period a patient receives a total of 300 days’ worth of medication, MPR = 300 / 365 = 82.2%.
Proportion of Days Covered (PDC)
PDC = (number of days within period when patient has medication on-hand) ÷ (number of days in the period) (4)
Example: A member receives a 30-day supply of a maintenance medication on January 1. They refill on February 5 with another 30-day supply. The first fill covers January 1 through January 30. The refill on February 5 extends coverage from January 31 through March 1. The member is without medication from January 31 through February 4, which creates a 5-day gap. Over a 60-day measurement period, they have medication available for 55 days. Their PDC is 55 divided by 60, which equals 91.6%.
Comparison of the two primary metrics used to measure medication adherence
What Happens When Employers / PBMs Don’t Prioritize Adherence
If a PBM or employer-sponsored plan focuses only on lowering drug spend through rebates, discounts, and formularies but ignores adherence, the expected savings often disappear.
Low adherence undermines drug effectiveness. Patients may skip doses or not refill at all due to cost or confusion. That undercuts the clinical value of the benefit design.
Poor adherence drives higher medical utilization. More hospitalizations, ER visits, complications from unmanaged chronic diseases. That increases overall plan costs.
Lost productivity. Employees missing work, using sick days or disability leave. For example, studies show that improving adherence among a population with diabetes can reduce short-term disability days significantly, saving employers real dollars. (5)
Waste: money spent on pharmacy benefit (drugs) that never deliver outcomes. If drugs are filled but not taken, the employer essentially paid for no clinical value.
Without adherence oversight, PBMs have little incentive to ensure refills translate into medication use, particularly when their revenue depends on dispensing volume or rebate maximization rather than outcomes.
A fiduciary PBM treats adherence as core to cost management. It monitors MPR and PDC, identifies members falling off therapy, addresses affordability barriers, and reports adherence trends transparently. Employers see fewer surprises in the medical plan and better outcomes across their population.
Sources:
HealthLinks Certified: Medication adherence guide
GoodRx: How affordability impacts adherence
Pharmacy Times: Differences between adherence measures
World Pharmacy Council: Best practices for measuring adherence
Michigan Public Health: Impact of adherence on health outcomes and disability
A decade of teaching pharmacy benefits distilled into five lessons that help employers take control of drug spending and strengthen fiduciary oversight.
When I started teaching pharmacy benefits, I assumed most people in HR, finance, and brokerage had a decent grasp of PBMs. Ten years in, I know better. What I see over and over is smart professionals trying to manage a multi-million dollar line item with incomplete information, opaque contracts, and vendors who are highly motivated to keep it that way.
Here are five hard lessons those ten years have driven home.
1) Most smart people don’t know what they don’t know about PBMs
I routinely teach people with 10, 15, even 20 plus years in benefits. Many walk into the first session thinking PBMs are just another vendor to benchmark on admin fees and rebates. By week two or three, the comments shift to some version of: “How have I managed pharmacy benefits this long without seeing any of this?”
The lesson: PBM literacy is far lower than most leaders realize. That is not an insult, it is a reality of an industry built on complexity and jargon. Until HR, finance, and advisors acknowledge that gap, they cannot close it. Once they see the full model, they stop treating pharmacy as a sidecar to medical and start managing it as a financial and clinical asset that deserves board-level attention.
2) The revenue model is the story, not the marketing
Every glossy PBM deck promises “lowest cost” and “industry leading rebates.” After teaching hundreds of students how the money actually moves through the system, I have yet to see a flashy rebate slide, for instance, that mattered more than the revenue model underneath it.
What changes behavior is understanding where the PBM actually gets paid: spread, retained rebates, manufacturer fees, network differentials, data monetization, and a stack of “miscellaneous” charges that are anything but. Once learners map those cash flows against their own claims data, they stop asking “What is your AWP discount?” and start asking “Show me every dollar you touch, keep, or re-route, and put that in the contract.”
The Lesson: if you cannot clearly and accurately explain your PBM’s revenue model to your CFO in one page, you are not operating at a fiduciary standard of care.
3) Contract language is a financial strategy, not legal cleanup
In almost every cohort, there is a moment when someone realizes their PBM contract is basically a revenue permission slip written in the PBM’s favor. Definitions are vague. Audit rights are weak. Ownership of data is unclear. “Guarantees” are riddled with carve-outs.
Over ten years teaching pharmacy benefits, I have learned that contracts are not a legal formality you hand to outside counsel at the eleventh hour. They are a primary cost containment tool. When HR, finance, and advisors learn how to specify fiduciary duties, define “lowest net cost,” lock in data rights, and eliminate gag clauses and side deals, the financial results change.
The lesson: leaders who treat PBM contracting as a strategic discipline, not a box to check, consistently get better pricing, better transparency, and cleaner audit trails. Leaders who do not, subsidize somebody else’s margin.
4) Plan design and clinical strategy beat rebate chasing every time
Most employers have been trained to chase rebates, copay cards, and “savings programs” while ignoring the engine that drives long-term cost: plan design paired with clinical strategy.
Ten years of case studies have shown me the same pattern. The plans that win:
Use formulary management to move members to effective, lower-net-cost therapies, not just to maximize rebates.
Align site-of-care and specialty strategies so J-code and specialty drugs are managed where utilization controls actually work.
Build cost sharing and utilization management rules that steer behavior instead of just shifting cost.
The lesson: HR and finance teams have far more control than they think, but it lives in plan rules and clinical policy, not in the renewal glossies. A fiduciary approach asks, “Does this design produce the lowest sustainable net cost and acceptable outcomes?” instead of “How big is the rebate check?”
5) Education is not a perk; it is a fiduciary duty
I used to think education was a nice value-add. A way to differentiate. After a decade of teaching, I see it differently. Education is infrastructure.
When an employer or consulting firm invests in real pharmacy benefits education, you can see the shift:
Their RFPs stop asking generic questions and start demanding specific disclosures and data files.
Their internal committees ask sharper questions, especially about specialty spend and vendor conflicts.
Their leaders document decisions and oversight in a way that would make any regulator, auditor, or plan member more comfortable.
The lesson: Staying uninformed about a multi-million-dollar drug plan is a choice that benefits someone else. A fiduciary standard requires you to understand the system, not rely on the PBM’s scoreboard.
Closing thought
Companies assume everyone has the same information, but knowing the right information and acting on it are very different. You gain advantage by analyzing the right information, understanding its impact, and executing a plan you can actually deliver.
After ten years of teaching pharmacy benefits, access to data or vendor promises does not drive the real differentiator. It’s the willingness to understand the system, apply fiduciary discipline, and make decisions that move the plan forward.
Elevate your expertise in pharmacy benefits management with the Certified Pharmacy Benefits Specialist® (CPBS) program. Whether you’re an HR leader, finance executive, consultant, or pharmacist, this certification provides the in-depth knowledge and strategic insight needed to manage pharmacy benefits with confidence and cost efficiency. Earn up to twenty continuing education credits while advancing your fiduciary and professional competencies. Both SHRM and HRCI accredit the CPBS program, which makes it a strong addition to your professional development portfolio. Strengthen your career, deliver measurable results, and help your organization take control of pharmacy spend. Register today to join a growing network of professionals shaping the future of pharmacy benefits management.
California’s new PBM fiduciary law has finally put into writing what it means to be a fiduciary PBM. PBMs that manage someone else’s money should be required to act in that person’s best interest. The law matters because prescription drug spending continues to rise, and most plans still operate with limited visibility into how their PBM gets paid, what incentives drive decisions, and whether those decisions help or hurt members.
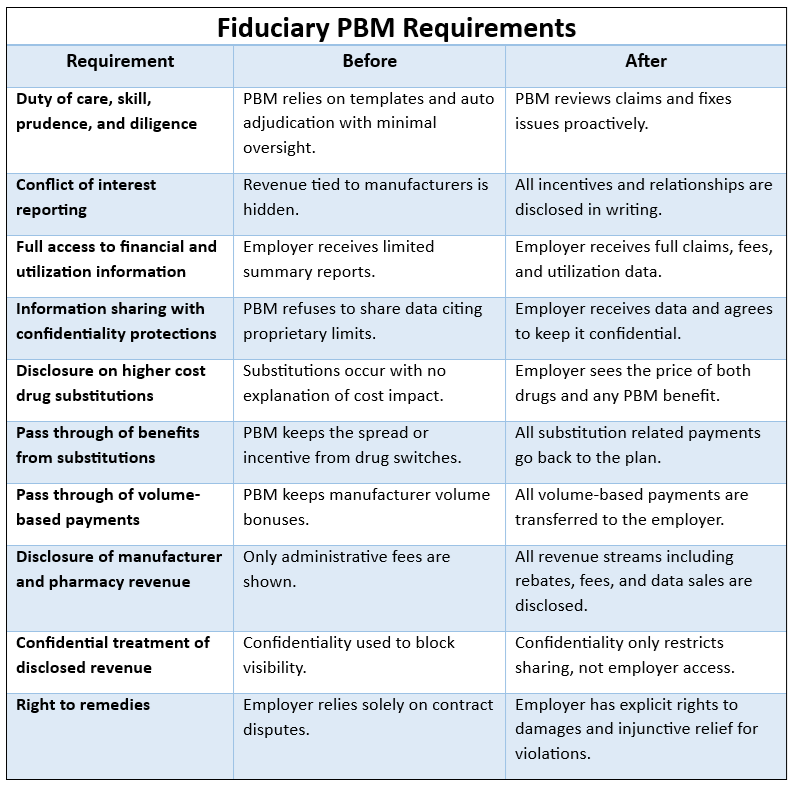
With this shift, employers and consultants have an opening to reset expectations. The moment demands clarity about what fiduciary PBM behavior looks like in day to day practice, not just in theory. Below is a breakdown of ten core requirements that define how a fiduciary PBM works, with short before and after examples and one verification step you can put in place for each.
1. Duty of Care, Skill, Prudence, and Diligence
Plain English: The PBM must run your plan as carefully as a reasonable expert would.
Before: The PBM relies on standard templates and auto adjudication with little interest in outcomes.
After: The PBM actively reviews claims patterns and fixes errors without being asked.
Verification: Require written documentation of quarterly clinical and financial oversight activities.
2. Conflict of Interest Reporting
Plain English: If the PBM has incentives that could influence decisions, they must tell you.
Before: Revenue streams tied to manufacturers are hidden, leaving employers blind to bias.
After: Every incentive is disclosed in writing so you know how the PBM makes money.
Verification: Add a contract clause requiring written disclosure within ten days of any new conflict.
3. Full Access to Financial and Utilization Information
Plain English: You get every data point you need to monitor spending and performance.
Before: Employers receive summary reports with limited detail.
After: Employers have access to detailed claims, fees, and utilization files.
Verification: Require raw claims files delivered in a standard format each month.
4. Information Sharing with Confidentiality Protections
Plain English: The PBM can mark data confidential, but can’t block your access to it.
Before: PBMs refuse to share pricing details citing “proprietary information.”
After: You receive the data and simply agree not to share it without permission.
Verification: Confirm that confidentiality language only restricts sharing, not access.
5. Disclosures on Higher Cost Drug Substitutions
Plain English: If the PBM swaps a prescription to a more expensive drug, they must tell you why and who benefits.
Before: Substitutions happen behind the scenes with unknown financial impact.
After: You see the price of both drugs plus any benefit the PBM receives.
Verification: Require a quarterly report showing all substituted drugs and financial flows.
Before / After Comparison Table
6. Passing Through Benefit from Substitutions
Plain English: If the PBM earns money from switching to generic or other alternatives, that money goes to you.
Before: The PBM keeps the spread or bonus tied to a substitution.
After: Every dollar tied to a substitution is returned to the plan.
Verification: Reconcile substitution payments against claims files to confirm full pass through.
7. Passing Through Volume Based Payments
Plain English: Any payment the PBM gets for driving volume to certain drugs must go to the plan.
Before: PBMs collect volume bonuses from manufacturers without employer knowledge.
After: All volume based compensation is transferred to the employer.
Verification: Require an annual manufacturer compensation statement signed by an officer.
8. Full Disclosure of Manufacturer and Pharmacy Revenue
Plain English: The PBM must show every way it makes money from manufacturers and pharmacies.
Before: Employers only see administrative fees listed in the contract.
After: Employers see network fees, formulary payments, rebates, data sales, and more
Verification: Require a schedule listing every revenue category tied to your plan.
9. Confidential Treatment of Disclosed Revenue
Plain English: You receive the information but agree to keep it confidential.
Before: PBMs use confidentiality claims to block transparency.
After: PBMs share the data and rely on a standard nondisclosure agreement.
Verification: Ensure the NDA protects PBM proprietary information without limiting oversight.
10. Right to Remedies
Plain English: If the PBM violates fiduciary duty, the plan can seek damages and injunctive relief.
Before: Employers rely solely on contract disputes with limited leverage.
After: Employers have clear legal recourse when the PBM breaches its obligations.
Verification: Confirm this right is explicitly written into your contract.
Critical Takeaways
A fiduciary PBM must show every dollar it earns from your plan and pass through anything tied to drug costs.
You should receive full access to claims data, pricing details, and manufacturer revenue.
Substitutions, conflicts, and incentives must be disclosed in plain language so you can verify alignment.
Conclusion
Fiduciary duty is not marketing language. It is an operating system that requires discipline, transparency, and hands on management. Most PBMs are not built for this level of accountability because it forces them to give up revenue streams they have depended on for years. Our organization pioneered the fiduciary standard of care in pharmacy benefits, long before California’s law, and we have spent years showing employers what it looks like in daily operations. If you want clarity, you need a partner that actually lives this model.
Author Bio
Tyrone Squires is Managing Director of TransparentRx, the first pharmacy benefit manager to operate under a true fiduciary standard of care. He trains benefit leaders nationwide on how to lower drug spend without sacrificing outcomes. If you want help assessing where your plan stands, reach out for a fiduciary readiness review.
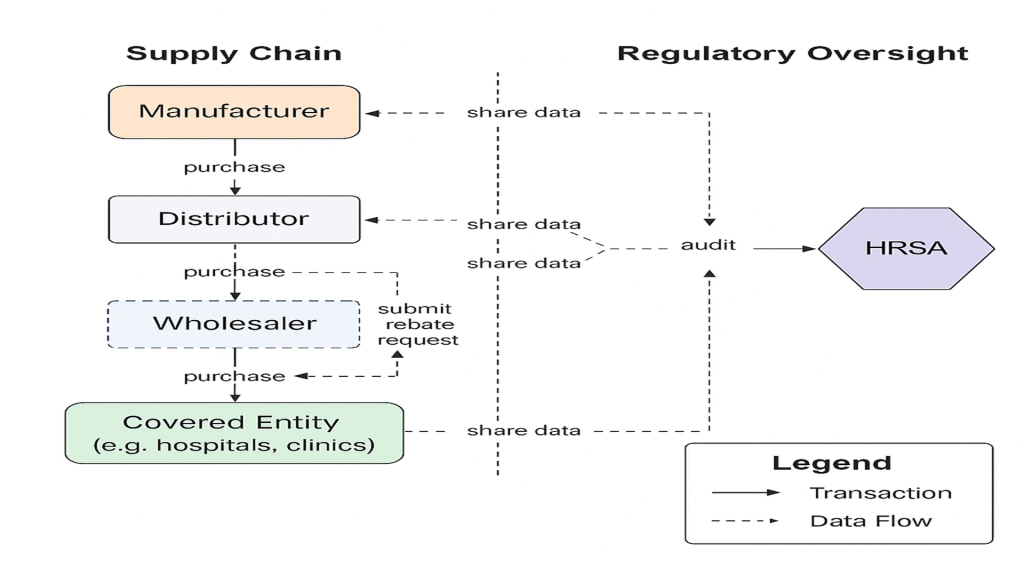
Relationships under the 340B Rebate Model Pilot Program, showing how data, rebates, and audit oversight flow.
The 340B Rebate Pilot Program turns the traditional 340B discount into a post-purchase rebate for select drugs, and plan sponsors need to assess how this shift may affect their pharmacy spend and oversight obligations. I suggest engaging with your PBM and reviewing contract language now.
What it is and why it was created
Launched by the Health Resources & Services Administration (HRSA) via a notice effective August 1 2025, the pilot invites manufacturers to offer rebates instead of upfront discounts under 340B for certain drugs tied to the Medicare Drug Price Negotiation list. (1)
The policy aims to address concerns over diversion, duplicate discounts and lack of timely claims-level data by requiring claim-data submissions before the rebate is paid. (2)
For plan sponsors and self-funded employers, the change matters because the financial mechanics and cash-flow for covered entities may shift and that may indirectly impact plan costs, especially if hospitals or other covered entities adjust pass-through pricing or contract pharmacy arrangements.
What it means for key stakeholders
Manufacturers They gain an option to provide 340B benefits via rebates rather than upfront discounts, which can improve visibility into how drugs are used under 340B and may reduce exposure to duplicate discounts. (3)
Action: Manufacturers will need to build IT platforms, collect multiple fields of claim data, and issue rebates within 10 calendar days of claim submission. (4)
PBMs/GPOs PBMs and group-purchasing organizations may face new operational overlays: verifying eligible claims, coordinating with wholesaler-accounts, and tracking rebate flows. The shift could affect how rebates are captured, passed along or retained.
Action: Review PBM contracts and audit pass-through language; ensure transparency of rebate disbursement mechanisms.
Plan Sponsors / Self-Funded Employers Your hospital or health system suppliers may in turn modify contract pharmacy flows, pricing structures, or pass-through arrangements under this pilot. Any disruption in discount pass-through could bounce back into plan cost.
Action: Request visibility into 340B-related rebates and contract pharmacy pricing with TPAs and PBMs now. Insert auditing language on 340B rebate mechanisms in vendor contracts.
Patients While covered entities retain the 340B benefit in theory, patients may feel indirect effects: if cash-flow or administrative burden on covered entities increases, there could be pressure to shift service settings or pharmacy sites. Some safety-net providers warn the rebate-model may strain operations. (5)
Action: Monitor patient access trends at your network pharmacies or contract pharmacy settings tied to 340B-entities.
Three key takeaways
The pilot makes upfront discounts into post-purchase rebates for select drugs under 340B, shifting cash-flow and requiring more claims-level data.
Plan sponsors should review and update contracts with PBMs/TPAs to preserve pass-through of 340B benefit and gain audit rights.
Early engagement and oversight on data workflows, claim submissions and vendor processes will protect your plan from hidden cost migration.
Conclusion and CTA This pilot isn’t about accusing anyone; it’s about staying ahead of a shift in how 340B savings might flow and ensuring the fiduciary standard of care for your health plan. If you’d like help unpacking your contracts, drafting data requests or assessing vendor readiness, let’s start that conversation.
Frier Levitt. “340B Alert: What You Need to Know About HRSA’s Rebate Pilot Program.”
Milliman. “340B Rebate Model Pilot Program—Medicaid implications and readiness.”
VytlOne. “HRSA 340B Rebate Model Pilot Program FAQs.”
Becker’s Hospital Review. “HRSA launches 340B rebate pilot with 8 drugmakers: 5 things to know.”
Elevate your expertise in pharmacy benefits management with the Certified Pharmacy Benefits Specialist® (CPBS) program. Whether you’re an HR leader, finance executive, consultant, or pharmacist, this certification provides the in-depth knowledge and strategic insight needed to manage pharmacy benefits with confidence and cost efficiency. Earn up to twenty continuing education credits while advancing your fiduciary and professional competencies. The CPBS program is accredited by both SHRM and HRCI, making it a powerful addition to your professional development portfolio. Strengthen your career, deliver measurable results, and help your organization take control of pharmacy spend. Register today to join a growing network of professionals shaping the future of pharmacy benefits management.
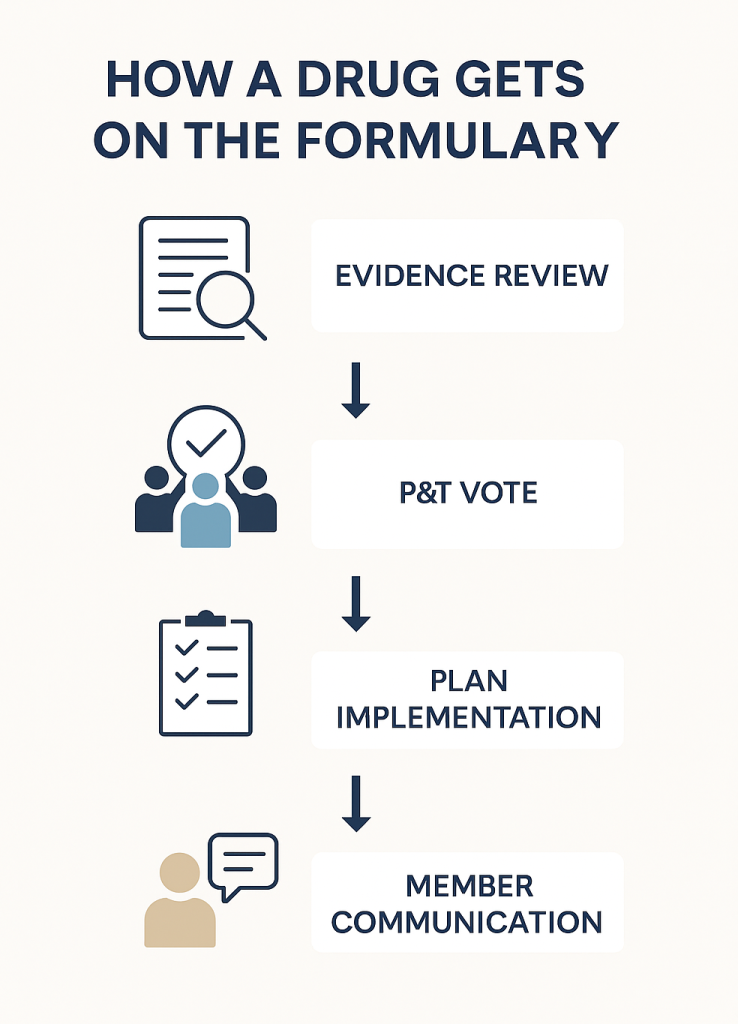
The Pharmacy and Therapeutics (P&T) Committee Finally Getting Their Flowers
When pharmacy benefits come up, formularies usually steal the spotlight. Yet behind every formulary sits a Pharmacy and Therapeutics (P&T) Committee, professionals quietly steering drug coverage decisions that shape both patient outcomes and plan results. For benefits leaders, understanding how these committees operate is critical to safeguarding plan integrity and member health. Your job isn’t to override their expertise, but to make sure your decisions strengthen, not weaken, the work they do.
What Is a Formulary and Why It Matters
A formulary is simply a list of prescription drugs covered by a health plan. But it is more than a list; it is a strategy. The formulary’s purpose is to ensure clinical appropriateness, manage cost, and safeguard patient safety. Drugs included on the formulary are those that have been vetted for effectiveness, safety, and value compared with alternatives.
Some critics claim formularies aren’t necessary, arguing that patients and prescribers should decide freely without restrictions. But that argument ignores reality. Every plan, drug management vendor, or coalition ultimately operates from a list of preferred drugs, whether they call it a formulary or not. The difference is transparency and intent. A fiduciary formulary is designed to serve the member and plan sponsor not to maximize rebates or profit margins.
For example, two cholesterol drugs may work equally well, but if one costs 40 percent less, the formulary will prefer that option unless there is a clinical reason not to. This keeps members on the most effective therapy at the lowest reasonable cost, a core principle of fiduciary oversight in pharmacy benefits.
The Role and Makeup of a P&T Committee
A P&T Committee is an independent panel of clinicians, typically pharmacists, physicians, and sometimes nurses, who evaluate scientific evidence to decide which medications should appear on the formulary. Members are selected based on clinical expertise and independence, not loyalty to a PBM or drug manufacturer.
Each member must disclose potential conflicts of interest, such as consulting fees or research grants from pharmaceutical companies. Strong governance practices require recusal from votes where a conflict exists. The committee’s deliberations are documented, and minutes are maintained to ensure transparency and accountability.
A typical committee might include a hospital pharmacist, an endocrinologist, a primary care physician, and a clinical pharmacologist. This mix ensures decisions are well-rounded, balancing specialty and primary care perspectives.
How P&T Committees Make Decisions
When evaluating a new drug, the P&T Committee relies on a structured, evidence-based process designed to balance clinical benefit with financial responsibility. A central tool in this process is the drug monograph, a concise yet comprehensive report summarizing all relevant data about a medication.
Behind every cost-effective, clinically sound formulary stands a disciplined process led by a P&T committee where evidence, ethics, and patient outcomes guide every decision.
Drug monographs are typically prepared by clinical pharmacists or analysts before each committee meeting. They include information on a drug’s mechanism of action, FDA-approved indications, dosing, contraindications, clinical trial outcomes, comparative efficacy, safety profile, and economic impact. Many committees also include a budget impact model and an assessment of real-world evidence, if available.
Using these monographs, the committee systematically reviews each therapy through five primary lenses:
Clinical efficacy – How well does the drug perform compared to existing alternatives?
Safety – What are the known risks, side effects, and contraindications?
Comparative effectiveness – Does the new therapy offer meaningful advantages over established treatments?
Guideline alignment – Is the drug recommended or supported by authoritative bodies such as the American Heart Association or National Comprehensive Cancer Network?
Economic value – What is the total cost of care, considering both drug price and downstream medical costs like hospitalizations or lab monitoring?
After reviewing the monograph and any supplemental materials, the committee engages in open discussion. Members may request clarification, additional data, or real-world utilization insights from PBM or plan analysts. Final decisions are made by vote or consensus, with results formally recorded in the meeting minutes.
Example: A P&T Committee once reviewed a new diabetes medication that promised improved glucose control. The monograph revealed that while early data looked favorable, the long-term studies showed no added benefit compared to existing agents, yet the cost was triple. Relying on the monograph’s evidence, the committee voted to exclude the drug from the formulary, avoiding unnecessary spend while maintaining clinical quality.
How External Forces Can Undermine the Process
Despite its rigor, the P&T process is not immune to outside pressure. Several factors can erode its integrity:
Rebate-driven formulary changes: Some PBMs may pressure committees to favor high-rebate drugs even when lower-cost equivalents are equally effective. This practice shifts savings from the plan sponsor to the PBM.
Manufacturer marketing: Drugmakers may inundate physicians or committee members with promotional materials that overstate benefits or underplay risks.
Plan design overrides: Employers or insurers sometimes introduce benefit designs that favor drugs not aligned with the formulary’s intent.
Member or prescriber appeals: When members or doctors appeal formulary exclusions based on personal preference rather than clinical necessity, consistent decision-making becomes difficult.
Each of these pressures threatens the committee’s independence and, by extension, the fiduciary duty employers owe their plan members.
How HR and Benefits Leaders Can Protect P&T Integrity
Protecting the committee’s work starts with strong governance and oversight. HR and finance leaders should see the P&T Committee as a safeguard for plan integrity, not a formality. The committee must operate independently from the PBM’s rebate and network teams, with members selected through a transparent process and governed by written bylaws that prevent conflicts of interest.
Documentation matters. Meeting minutes, voting records, and decision rationales should be retained and easily accessible. These records demonstrate fiduciary care and ensure that coverage decisions are based on objective evidence, not financial influence.
Employers also need to confirm that P&T decisions align with plan design yet remain insulated from rebate negotiations. When PBMs allow financial motives to shape clinical judgment, the process loses credibility.
Clear communication with plan members is equally critical. Employees deserve to know why certain drugs are covered and others are not. Transparency builds trust and minimizes confusion over cost-sharing or exclusions.
Lastly, benefits teams need regular training to understand formularies, drug tiers, and PBM reports. This knowledge helps them spot misalignment and reinforces the committee’s work. Strong governance, transparency, and education together ensure that the P&T Committee’s decisions protect both plan integrity and member health.
Practical Checklist: Safeguarding the P&T Process
Verify the P&T Committee’s independence and review its bylaws annually.
Require conflict-of-interest disclosures from all committee members.
Audit a sample of formulary decisions each year to confirm documentation and rationale.
Include P&T governance standards in PBM contracts and service-level agreements.
Provide plan members with transparent communication about formulary updates.
Call to Action
Pharmacy and Therapeutics Committees are the quiet guardians of clinical and financial integrity in pharmacy benefits. Employers and HR leaders who understand their importance can prevent waste, avoid conflicts of interest, and keep members safe. Now is the time to review your PBM’s P&T governance structure, verify its independence, and ensure every formulary decision serves one goal: better care, cost-effectively.
Elevate your expertise in pharmacy benefits management with the Certified Pharmacy Benefits Specialist® (CPBS) program. Whether you’re an HR leader, finance executive, consultant, or pharmacist, this certification provides the in-depth knowledge and strategic insight needed to manage pharmacy benefits with confidence and cost efficiency. Earn up to twenty continuing education credits while advancing your fiduciary and professional competencies. The CPBS program is accredited by both SHRM and HRCI, making it a powerful addition to your professional development portfolio. Strengthen your career, deliver measurable results, and help your organization take control of pharmacy spend. Register today to join a growing network of professionals shaping the future of pharmacy benefits management.
Half-truths and hidden agendas drive up costs. Understanding how misinformation spreads in pharmacy benefits is the first step toward protecting your plan and your members.
Every week, I hear well-meaning brokers, consultants, and HR leaders repeat things they have been told about pharmacy benefits that simply aren’t true or misleading. The problem is not ignorance; it is misinformation. PBMs and others in the supply chain often frame partial truths as facts to protect their margins and maintain control. Employers are the ones paying for it.
Let’s look at four examples that show how misinformation spreads and why it costs plan sponsors billions.
The 340B Misconception
A broker recently asked me, “We’ve heard that by the time the plan sponsor pays for a 340B drug, the hospital and dispensing pharmacy have inflated the price so much that the savings are gone. Is that true?”
It is not. Look at the data from our 340B portal. Across dozens of high-cost specialty drugs, the 340B price including shipping still comes in well below the ingredient cost in retail channels. For example, drugs like Creon and Genotropin show plan-level savings of $1,900 to $5,800 per claim under 340B pricing. Even for the highest-cost biologics like Skyrizi, savings exceed $7,000 per claim.
Specialty drugs often deliver much higher 340B savings than small-molecule brands.
So where does this “no savings” narrative come from? It is a deflection. Drugmakers, hospitals, and PBMs all have financial interests in keeping plan sponsors away from 340B opportunities. The fewer questions employers ask, the easier it is for intermediaries to capture those margins.
The Contract Deflection
Another broker posted on LinkedIn a PBM said to him, “Why does our contract matter if we’re guaranteeing your spend?”
That is classic misdirection. PBMs use “guarantees” to distract from contract language that controls how much money they keep. Spend guarantees sound like protection, but they do not change the underlying math. The contract defines what is included or excluded from that spend. Rebates, administrative fees, clinical programs, and manufacturer revenue all hide behind those clauses.
A guarantee means nothing if it is built on a bad foundation. A fiduciary PBM contract, by contrast, gives employers visibility into every revenue stream and audit right. That is the only way to ensure your “guarantee” is based on real savings, not financial engineering.
The NADAC Oversimplification
A consultant pharmacist posted on LinkedIn, “Generic drug costs dropped 17 percent on average over the last five years, but PBM contract prices went up…This is why NADAC is compelling for contracting.”
It sounds logical but it is misleading. NADAC represents the average acquisition cost to the pharmacy, not the total cost to dispense a prescription. When you add professional dispensing fees of ten to twenty-five dollars per prescription, the NADAC model starts to fall apart as a savior for drug pricing.
Using NADAC in isolation ignores the economics of the transaction. Employers that buy into this argument often find themselves paying more overall once the fees, spreads, and administrative costs are added in. Transparency without context is not transparency; it is marketing.
The MTM Misunderstanding
On the popular Healthcare Benefits Hackers Google Group, a consultant responded to this post: “Some pass-throughs offer value-based formularies (rather than rebate-driven formularies), which reduces spend by favoring lower-cost drugs when several drugs have equivalent clinical value in a given therapeutic category.”
The consultant replied, “Our generic procurement process significantly minimizes the need for MTM programs within a therapeutic class because the pricing delta between drugs in the same therapeutic class is minimal.” That response conflates drug pricing with drug use, and that is where the logic falls apart.
MTM is not about price; it is about appropriateness and outcomes. Medication Therapy Management targets misuse, duplication, and non-adherence, not just the unit cost of drugs. Even if the pricing spread within a class is narrow, inappropriate utilization such as wrong dose, duplicate therapy, or unnecessary combinations drives waste. A low-cost drug used incorrectly is still a waste of plan dollars and harms patient outcomes.
Generic procurement does not address polypharmacy, adherence, or contraindications. Buying generics efficiently is good practice but does nothing to prevent a diabetic patient from taking five overlapping medications from three prescribers. MTM catches these scenarios before they cause harm or hospitalization. Procurement does not.
Therapeutic classes are not monolithic. Even when drugs are in the same class, differences in pharmacokinetics, patient comorbidities, and side effect profiles can make one option far more cost-effective in practice. MTM accounts for clinical effectiveness in real patients, not theoretical cost equivalence.
Minimal price delta does not mean minimal risk. Many expensive claims stem from misuse of “cheap” drugs that lead to hospitalizations or new prescriptions for side effects. MTM prevents these downstream costs, which procurement cannot touch.
Value-based formularies and MTM are complementary, not substitutes. A value-based formulary optimizes which drugs are available. MTM ensures they are used correctly. One sets the table, the other keeps the meal balanced. Suggesting one replaces the other ignores how comprehensive cost control actually works.
In short, claiming “we don’t need MTM because our pricing is good” is like saying “we don’t need seatbelts because our cars have good brakes.” It misses the point and leaves the plan, and its members, exposed.
Taking Back Control
HR and benefits leaders cannot rely on assumptions or industry hearsay. The only way to protect plan assets is through education. When you understand the mechanics of PBM contracts, plan design, clinical programs, and pricing models, you stop chasing marketing claims and start demanding accountability.
Informed leaders pay less, get better outcomes, and get a seat on the board of directors. Uninformed ones overspend, accept conflicts of interest, and wonder why they get passed over for promotions.
A recent CPBS student said it best:
“From a consultant’s perspective, none of my clients or prospective clients have any clue what BER, GER, and similar terms even mean. That makes the way this exam is structured completely disconnected from the reality of what consultants actually do.”
That gap in understanding is exactly why misinformation thrives and why education remains the most powerful antidote.
Elevate your expertise in pharmacy benefits management with the Certified Pharmacy Benefits Specialist® (CPBS) program. Whether you’re an HR leader, finance executive, consultant, or pharmacist, this certification provides the in-depth knowledge and strategic insight needed to manage pharmacy benefits with confidence and cost efficiency. Earn up to twenty continuing education credits while advancing your fiduciary and professional competencies. The CPBS program is accredited by both SHRM and HRCI, making it a powerful addition to your professional development portfolio. Strengthen your career, deliver measurable results, and help your organization take control of pharmacy spend. Register today to join a growing network of professionals shaping the future of pharmacy benefits management.
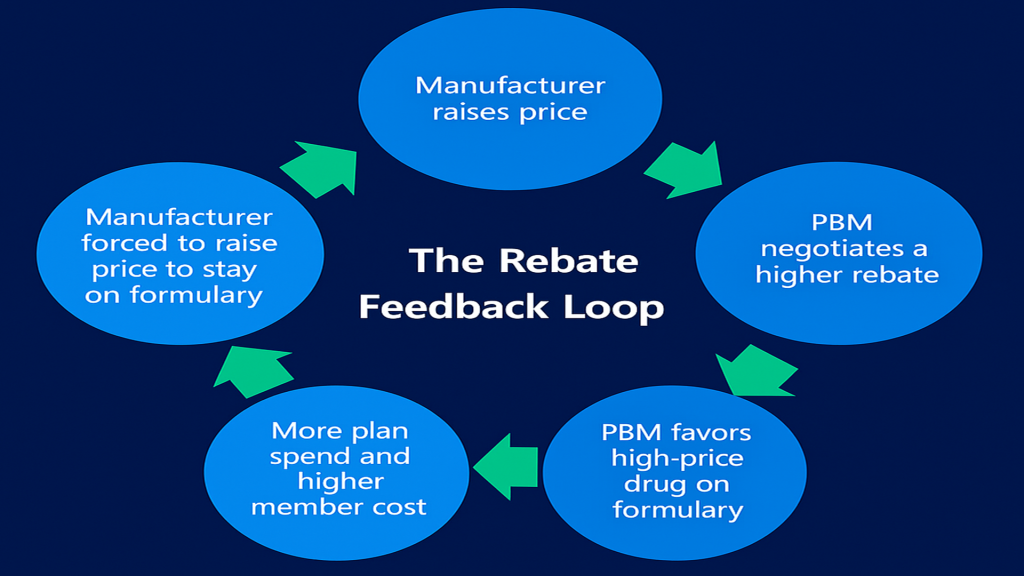
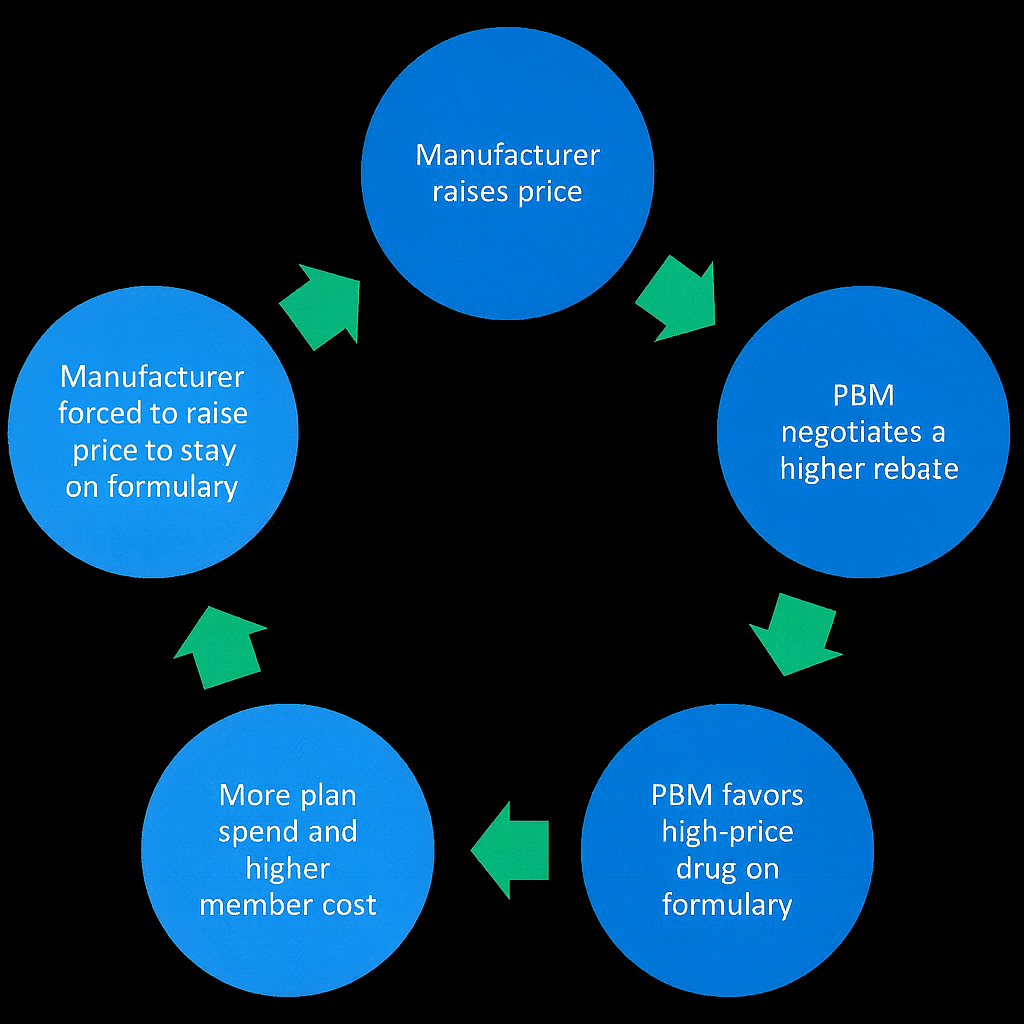
Imagine a circular track where every participant, including the drug manufacturer, PBM, and plan sponsor, is running hard but not moving forward. That is the 360-degree rebate feedback loop. It begins with the intent to control costs but often leads to higher drug prices, increased plan spend, and more out-of-pocket costs for members.
In this loop, a manufacturer raises a drug’s list price to fund larger rebates. The PBM negotiates higher rebate payments and favors those higher-priced drugs on its formulary. The plan ends up paying more at the point of sale, while the PBM collects a larger rebate or spread behind the scenes. Manufacturers, trying to stay competitive, raise prices again to maintain access, and the cycle repeats.
When plan sponsors focus only on rebate size instead of the economics behind it, the loop strengthens. The result is an illusion of savings that masks a growing total cost of pharmacy care (TCoPC).
Why Transparency Matters
True transparency in rebates means more than receiving a flat “rebate guarantee per script.” It means understanding where rebates originate, how they are calculated, and how much is retained by intermediaries such as PBMs, rebate aggregators, or manufacturer-affiliated entities.
Opaque rebate arrangements often hide spreads and misaligned incentives. For example, if a PBM secures $200 per claim from a manufacturer but only passes $150 to the plan sponsor, the $50 difference becomes a silent profit center. Without clear documentation and audit rights, that gap remains invisible.
Transparency ensures that plan sponsors can trace every dollar from manufacturer to member, revealing who benefits and who pays. It brings the entire rebate value chain into focus and exposes what is commonly called the Gross-to-Net (GTN) gap.
The Hidden Margin
The GTN gap is the difference between a drug’s list price (gross) and what manufacturers actually realize after all rebates, fees, and discounts (net). For many brand drugs, this gap can exceed 50 percent. Manufacturers inflate list prices to accommodate larger rebates and retain formulary access, while PBMs market those rebates as plan savings. In reality, both the plan and its members pay higher prices upfront to fund the rebate economy.
Understanding GTN is essential for employers because it reveals the disconnect between what is billed and what is truly paid. Closing the GTN gap through full transparency can directly reduce total plan costs and improve member affordability.
Turning the Loop into a Closed System
A closed-loop rebate process works like a well-calibrated thermostat that measures, tracks, and adjusts. When rebate data flows openly back to the plan sponsor, employers can make smarter formulary decisions that prioritize clinical value over rebate size.
This type of process increases generic dispensing rates, optimizes formulary design, and drives measurable improvement in overall plan performance. It shifts the focus from maximizing rebate yield to reducing the total cost of pharmacy care.
Competitive Advantage Through Clarity
Transparency should not be viewed as a compliance requirement. It is a competitive advantage. Employers who understand their PBM’s rebate model can negotiate from a position of strength, identify hidden costs, and build pharmacy benefits that align with fiduciary responsibility.
In a market where healthcare inflation and specialty drug costs continue to climb, clarity is not optional. It is essential to long-term sustainability. A transparent rebate structure not only builds trust but also allows employers to turn data into strategic leverage by controlling costs and improving outcomes over time.
What Employers Should Do
Ask your PBM to provide documentation that clearly traces rebate sources and cash flows through every step of the value chain. A truly transparent PBM relationship should help you:
Avoid rebate aggregator formularies. These often add another opaque layer that dilutes value and complicates auditability.
Achieve a 91%–93% generic dispense rate (GDR). A strong GDR is one of the most reliable indicators of effective formulary management and cost efficiency.
Limit eligibility exclusions that reduce rebate yield. Overly restrictive eligibility rules can block your plan from capturing legitimate rebate value.
Eliminate conflicts of interest. Your PBM should act solely in your plan’s best interest, with no hidden financial incentives that distort formulary decisions.
If your PBM cannot meet these standards, the rebate feedback loop is likely working against you, not for you.
Bottom line
The rebate feedback loop will persist until employers demand full visibility into how rebates are earned, shared, and retained. Closing that loop allows plan sponsors to reduce costs, improve member outcomes, and ensure every rebate dollar serves the plan’s best interest rather than the middlemen.
When PBMs operate without fiduciary duty, employees and their families pay the price through inflated drug costs, hidden fees, and limited access to affordable medications. TransparentRx takes a different approach. As a fiduciary PBM, we are legally bound to act in your best interest eliminating conflicts of interest, disclosing every dollar, and focusing on better adherence and outcomes. Partner with TransparentRx to ensure your pharmacy benefits strategy delivers real value where it matters most: at the point of care.
Group Purchasing Organizations (GPOs) often market their rebate aggregator programs as tools to deliver greater savings through scale. These structures can create opaque rebate spreads that inflate costs for plan sponsors while enriching intermediaries. Employers and consultants who understand how these spreads form and how to counter them can protect their plans from hidden markups.
The Rebate Feedback Loop
1. Avoid Use of Rebate Aggregator Formularies
A rebate aggregator formulary is a prepackaged drug list built around maximizing rebates instead of minimizing net cost. These formularies are typically managed by the GPO or its contracted PBM and emphasize drugs that deliver high rebate dollars rather than clinical or financial efficiency.
For example, an aggregator might favor a brand drug that pays a $200 rebate even though a generic alternative costs $300 less per fill. While the GPO and PBM split the rebate revenue, the plan sponsor ultimately pays more in total net cost.
Trade-offs
Pros: Larger rebate checks and a perception of “shared savings.”
Cons: Weaker clinical oversight, higher net plan costs, and misaligned incentives where formulary placement favors rebate-rich drugs instead of clinically superior or lower-cost options.
Better Approach Employers can insist on an independent formulary managed under a fiduciary PBM model. This ensures that rebate and formulary decisions are made based on clinical value and lowest net cost, not the PBM’s or aggregator’s revenue objectives. Fiduciary PBMs contractually commit to passing through 100 percent of rebates and disclose all revenue sources, giving employers full visibility into pricing and rebate flow.
2. Achieve a 91% – 93% Generic Dispense Rate (GDR)
A high Generic Dispense Rate (GDR) directly limits rebate spread opportunities. Rebate spreads thrive on brand utilization; every time a brand is dispensed over a clinically equivalent generic, the PBM or aggregator earns more rebate margin while the plan sponsor pays more.
When a plan consistently dispenses generics, especially in chronic care categories such as hypertension, cholesterol, and mental health, the volume of high-rebate brand claims falls, shrinking the room for rebate manipulation.
How to Improve GDR
Formulary design: Exclude brands where a generic is clinically appropriate.
Real-time benefit tools: Give prescribers visibility into cost-effective alternatives during prescribing.
Member engagement: Communicate savings opportunities through digital nudges, pharmacist counseling, and plan education.
Key Takeaway Chasing rebates at the expense of GDR is a losing strategy. A plan with 91% GDR and minimal rebates will nearly always outperform a plan with 85% GDR and “big rebate guarantees.” A higher GDR means fewer rebate-driven brand drugs and a cleaner, more efficient drug spend while maintaining the access needed for better health outcomes.
3. Limit Eligibility Exclusions That Undermine Rebate Access
PBMs and aggregators often use technical exclusions to withhold rebates that should belong to the plan. Common tactics include coding claims as “Dispense As Written” (DAW) or using step therapy rules that push a claim outside the rebate-eligible definition.
Example Suppose a plan member fills a high-cost brand drug coded as DAW 1, meaning the prescriber requested no substitution. If the PBM’s rebate contract defines this as “non-rebate eligible,” the plan loses the rebate even though the PBM still collects it from the manufacturer. That difference becomes spread revenue.
Countermeasures
Tight contract language: Define rebate eligibility broadly to include all formulary brand claims, regardless of DAW or utilization management flags.
Audit regularly: Review rebate remittance reports and identify discrepancies between paid claims and rebate payments.
Reconcile quarterly: Require detailed rebate reconciliations comparing manufacturer invoices to plan-level data to prevent leakage.
These measures ensure that the plan, not the PBM or aggregator, captures the full rebate value generated by its members’ utilization.
Final Thoughts
Employers must stop measuring PBM performance by rebate guarantees and start focusing on net cost integrity. Rebate aggregator models often convert transparency into opacity, masking spreads that work against plan sponsors. By rejecting rebate-driven formularies, driving generic use, and policing rebate eligibility, employers can regain control of their pharmacy spend and align incentives with their fiduciary duty. The best defense against rebate spreads is not a bigger rebate. It is a transparent, data-driven PBM relationship that prioritizes the plan’s financial and clinical outcomes over rebate revenue.
If you are a director of benefits seeking more control and clarity in your pharmacy program, TransparentRx can help you achieve it with confidence. As a fiduciary PBM, we align our interests with yours to deliver accountability, measurable savings, and better outcomes for plan members. Learn how our fiduciary approach supports informed decision-making and long-term value. Schedule a brief discovery call to explore how transparency can strengthen your benefit strategy.
Pharmacy benefits management is full of technical terms that can obscure critical details about pricing, utilization, and outcomes. For Benefits Leaders, understanding the right terminology is essential to managing risk, identifying hidden costs, and ensuring value for employees. Here are 10 Pharmacy Benefits Terms Everyone Should Know.
1. MAC Effective Rate (MER)
The Maximum Allowable Cost (MAC) list sets the reimbursement limit for generics. The MAC Effective Rate reflects the blended reimbursement across all MAC lists a PBM uses. Because PBMs can manipulate these lists to pad margins, monitoring your plan’s MER ensures you’re paying fair and predictable prices for generics. Many PBMs advertise extremely aggressive MAC Effective Rates (such as AWP minus 80% or more).
What they often fail to disclose is that these rates are tied to a narrow MAC list that covers only a small subset of generics most commonly dispensed to members. For the remainder of generic drugs, those excluded from the list, the PBM charges the plan sponsor at much weaker discounts (for example, AWP minus 15–20%). This practice significantly increases spread revenue for the PBM while making the “headline” MAC rate misleading.
2. Generic Substitution Rate (GSR)
This measures how often brand-name prescriptions are replaced with clinically equivalent generics. A high substitution rate is critical for cost control and should be 98% or better. For plan sponsors, tracking this metric shows whether cost-saving opportunities are being maximized or if employees are being steered toward more expensive options.
3. Medication Possession Ratio (MPR)
A key measure of medication adherence, MPR calculates the proportion of time a patient has access to their medication. An effective plan should target an MPR of 80% or better. Strong adherence reduces hospitalizations and overall healthcare costs.
Adherence rate is the single most important metric to determine if a pharmacy benefit manager is truly delivering value. High adherence indicates that patients are staying on therapy, which improves outcomes and lowers total medical spend.
Poor adherence rates, however, are a red flag. They often signal that the PBM is prioritizing claims processing over clinical outcomes, focusing on transactions rather than patient health. For Benefits Directors, tracking MPR alongside other metrics helps reveal whether your PBM is aligned with long-term organizational goals or simply moving claims through the system.
4. Rebate Yield
Rebate yield is the percentage of rebates retained relative to total drug spend. It should be at least 20% of brand drug spend. Monitoring rebate yield is critical for determining whether your PBM contract aligns with your organization’s financial goals.
5. Prior Authorization Approval Rate
This metric measures how often prior authorization (PA) requests are approved by the PBM. While the benchmark should generally be below 65%, the approval rate itself tells a deeper story about how the PA program is functioning.
High approval rates (e.g., 75% or higher) may indicate that:
Overly broad PA requirements are in place, forcing prescribers to submit unnecessary paperwork for therapies that are ultimately approved anyway. This creates administrative burden without meaningful cost containment.
The PBM may be using PA as a “speed bump” to generate revenue from administrative fees rather than as a clinical safeguard.
The PA criteria could be poorly aligned with evidence-based guidelines, resulting in friction but little actual clinical or financial value.
Low approval rates (e.g., below 50%) may indicate that:
The PBM is using PA too aggressively, potentially denying access to therapies that are medically necessary. This can frustrate patients and prescribers, lead to delays in treatment, and increase overall healthcare costs if patients deteriorate clinically.
The criteria for approval may be misaligned with current standards of care, forcing appeals or switches that add unnecessary complexity.
Denials may be used to steer patients toward preferred therapies or PBM-owned specialty pharmacies, prioritizing revenue over patient outcomes.
Balanced approval rates (ideally in the 50–60% range) suggest that:
The PA process is being applied selectively to high-cost or high-risk therapies where clinical oversight is warranted.
The criteria are evidence-based and designed to ensure safety, efficacy, and value without overburdening providers or patients.
The PA program is contributing to cost containment and care quality rather than serving as a profit lever.
6. Medication Therapy Management (MTM)
MTM programs ensure patients, especially those with multiple chronic conditions, are on the right medications and taking them correctly. Features of a good MTM program include:
Comprehensive medication reviews
Personalized action plans for patients
Drug interaction and duplication checks
Follow-up interventions to ensure adherence
Coordination with prescribers and pharmacists
For employers, MTM translates into lower claims, healthier employees, and fewer avoidable medical costs.
7. Specialty Dispensing Rate
Specialty drugs account for the majority of pharmacy spend. The specialty dispensing rate measures (as a percentage) how often prescriptions for these high-cost drugs are filled by PBM-owned or preferred specialty pharmacies. Since PBMs often mark up these fills, plan sponsors must monitor this rate to ensure that utilization is clinically necessary and cost-efficient.
It is also critical to pay close attention to how the PBM defines a “specialty drug.” Some PBMs use overly broad or vague definitions, which gives them the ability to classify almost any medication as “specialty.” This practice inflates costs and funnels prescriptions into higher-priced dispensing channels. A well-structured contract should limit the definition of specialty drugs to those that truly warrant the classification, based on cost, complexity, or storage/handling requirements.
8. Back-Billing
Back-billing occurs when PBMs withhold reimbursement to the pharmacy after the point of sale and keep those dollars without disclosing or sharing them with the plan sponsor. This hidden practice inflates PBM profits while reducing transparency. Benefits leaders should ensure their contracts prohibit back-billing and require disclosure of all revenue streams.
Real-Life Example of Back-Billing
9. Pharmacogenomics (PGx)
The study of how a person’s genes influence drug effectiveness and safety. Pharmacogenomic testing has the potential to reduce trial-and-error prescribing, improve patient outcomes, and lower costs by avoiding ineffective medications. While adoption is still growing, it is a trend worth watching. A good pharmacogenomics program for self-insured employers is built on clinical integration, employee engagement, strong data management, measurable outcomes, and fiduciary alignment.
Testing should follow evidence-based guidelines such as CPIC and FDA labeling, with results incorporated directly into prescribing workflows so that physicians, pharmacists, and care managers can act on them in real time. The program should focus on drug classes with the highest risk for gene–drug interactions, such as antidepressants, opioids, oncology, cardiovascular, and pain management therapies. Equally important is making the program accessible and meaningful for employees.
10. Total Cost of Pharmacy Care (TCoPC)
This term looks beyond the unit cost of prescriptions and considers the full impact of pharmacy care on the health plan. TCoPC includes every dollar spent associated with offering a pharmacy benefit program including but not limited to ingredient costs, claims management services, clinical services, medical costs avoided such as hospitalizations, and overall patient outcomes. For Directors of Benefits, this is an most important measure because it shows whether your pharmacy strategy is reducing total health spend, not just shifting costs.
? Takeaway for Benefits Leaders: You don’t need to be a pharmacist to oversee your PBM effectively, but you do need fluency in its language. Knowing these terms equips you to ask sharper questions, identify misaligned incentives, and ensure your organization’s pharmacy benefit dollars are working for your employees, not your PBM.
When pharmacy benefit managers operate without fiduciary responsibility, it’s employees and their families who suffer. Non-fiduciary PBMs often hide revenue streams, inflate drug costs, and steer members toward therapies that maximize their own profits rather than improve patient outcomes. The result? Higher out-of-pocket costs, barriers to cost-effective medications, and worse health outcomes for your workforce.
TransparentRx is different. As a fiduciary PBM, we are contractually bound to put your organization and your employees first. We eliminate conflicts of interest, disclose every dollar, and focus on driving true adherence and better health. Because when your employees can afford and access the medications they need, your company wins with healthier, more productive people.
Protect your employees from the hidden harm of non-fiduciary PBMs. ? Partner with TransparentRx and ensure your pharmacy benefits strategy delivers value where it matters most—at the point of care.
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.