Pharmacy & Therapeutics Committee: The Unsung Heroes of Pharmacy Benefits

When pharmacy benefits come up, formularies usually steal the spotlight. Yet behind every formulary sits a Pharmacy and Therapeutics (P&T) Committee, professionals quietly steering drug coverage decisions that shape both patient outcomes and plan results. For benefits leaders, understanding how these committees operate is critical to safeguarding plan integrity and member health. Your job isn’t to override their expertise, but to make sure your decisions strengthen, not weaken, the work they do.
What Is a Formulary and Why It Matters
A formulary is simply a list of prescription drugs covered by a health plan. But it is more than a list; it is a strategy. The formulary’s purpose is to ensure clinical appropriateness, manage cost, and safeguard patient safety. Drugs included on the formulary are those that have been vetted for effectiveness, safety, and value compared with alternatives.
Some critics claim formularies aren’t necessary, arguing that patients and prescribers should decide freely without restrictions. But that argument ignores reality. Every plan, drug management vendor, or coalition ultimately operates from a list of preferred drugs, whether they call it a formulary or not. The difference is transparency and intent. A fiduciary formulary is designed to serve the member and plan sponsor not to maximize rebates or profit margins.
For example, two cholesterol drugs may work equally well, but if one costs 40 percent less, the formulary will prefer that option unless there is a clinical reason not to. This keeps members on the most effective therapy at the lowest reasonable cost, a core principle of fiduciary oversight in pharmacy benefits.
The Role and Makeup of a P&T Committee
A P&T Committee is an independent panel of clinicians, typically pharmacists, physicians, and sometimes nurses, who evaluate scientific evidence to decide which medications should appear on the formulary. Members are selected based on clinical expertise and independence, not loyalty to a PBM or drug manufacturer.
Each member must disclose potential conflicts of interest, such as consulting fees or research grants from pharmaceutical companies. Strong governance practices require recusal from votes where a conflict exists. The committee’s deliberations are documented, and minutes are maintained to ensure transparency and accountability.
A typical committee might include a hospital pharmacist, an endocrinologist, a primary care physician, and a clinical pharmacologist. This mix ensures decisions are well-rounded, balancing specialty and primary care perspectives.
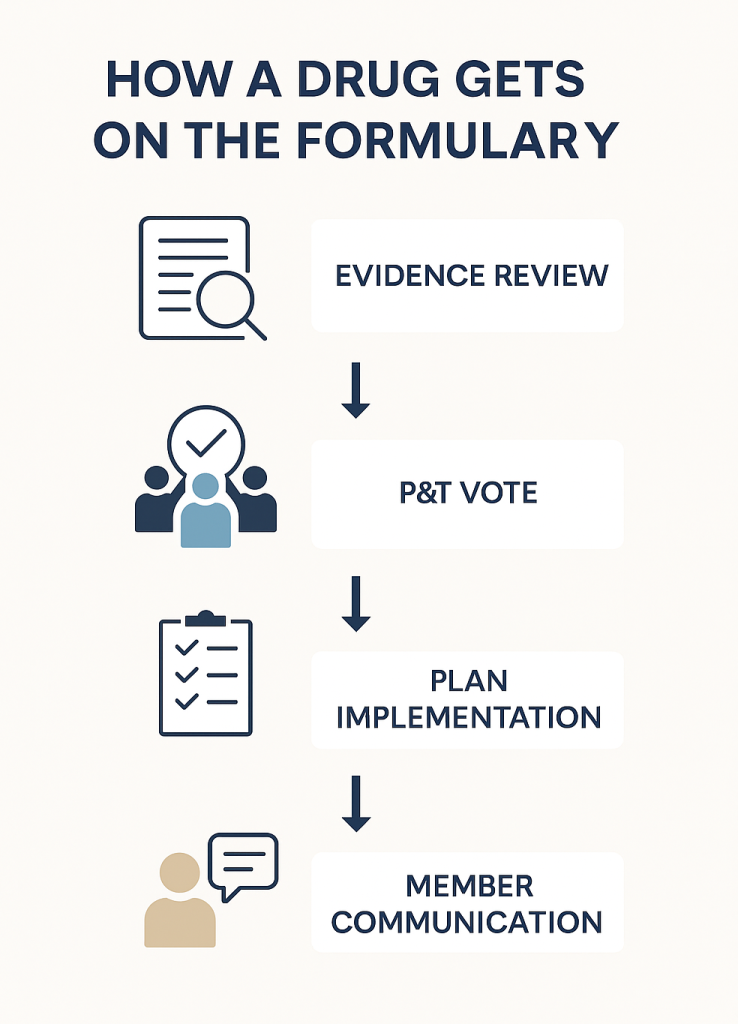
How P&T Committees Make Decisions
When evaluating a new drug, the P&T Committee relies on a structured, evidence-based process designed to balance clinical benefit with financial responsibility. A central tool in this process is the drug monograph, a concise yet comprehensive report summarizing all relevant data about a medication.
Drug monographs are typically prepared by clinical pharmacists or analysts before each committee meeting. They include information on a drug’s mechanism of action, FDA-approved indications, dosing, contraindications, clinical trial outcomes, comparative efficacy, safety profile, and economic impact. Many committees also include a budget impact model and an assessment of real-world evidence, if available.
Using these monographs, the committee systematically reviews each therapy through five primary lenses:
- Clinical efficacy – How well does the drug perform compared to existing alternatives?
- Safety – What are the known risks, side effects, and contraindications?
- Comparative effectiveness – Does the new therapy offer meaningful advantages over established treatments?
- Guideline alignment – Is the drug recommended or supported by authoritative bodies such as the American Heart Association or National Comprehensive Cancer Network?
- Economic value – What is the total cost of care, considering both drug price and downstream medical costs like hospitalizations or lab monitoring?
After reviewing the monograph and any supplemental materials, the committee engages in open discussion. Members may request clarification, additional data, or real-world utilization insights from PBM or plan analysts. Final decisions are made by vote or consensus, with results formally recorded in the meeting minutes.
Example: A P&T Committee once reviewed a new diabetes medication that promised improved glucose control. The monograph revealed that while early data looked favorable, the long-term studies showed no added benefit compared to existing agents, yet the cost was triple. Relying on the monograph’s evidence, the committee voted to exclude the drug from the formulary, avoiding unnecessary spend while maintaining clinical quality.
How External Forces Can Undermine the Process
Despite its rigor, the P&T process is not immune to outside pressure. Several factors can erode its integrity:
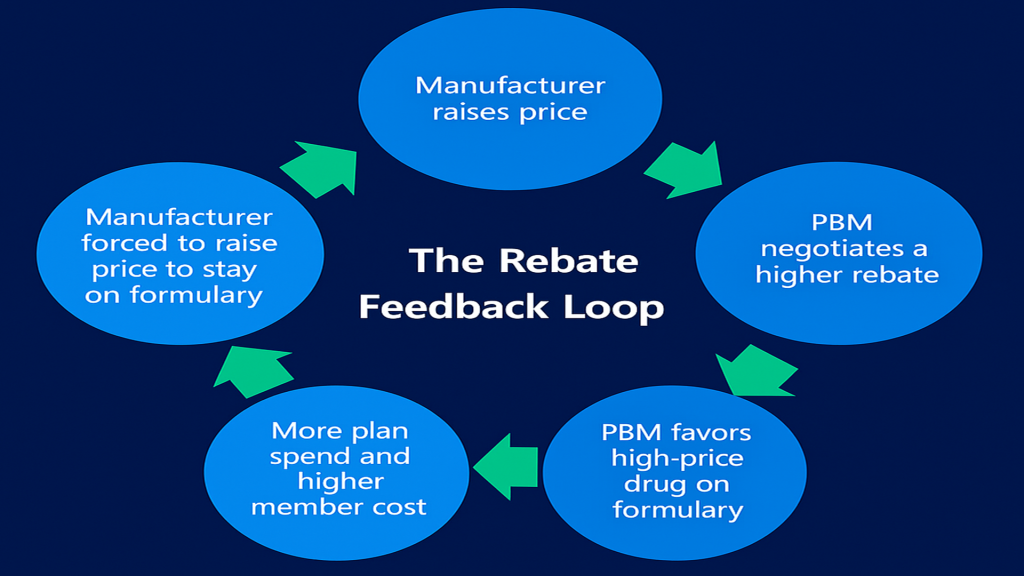
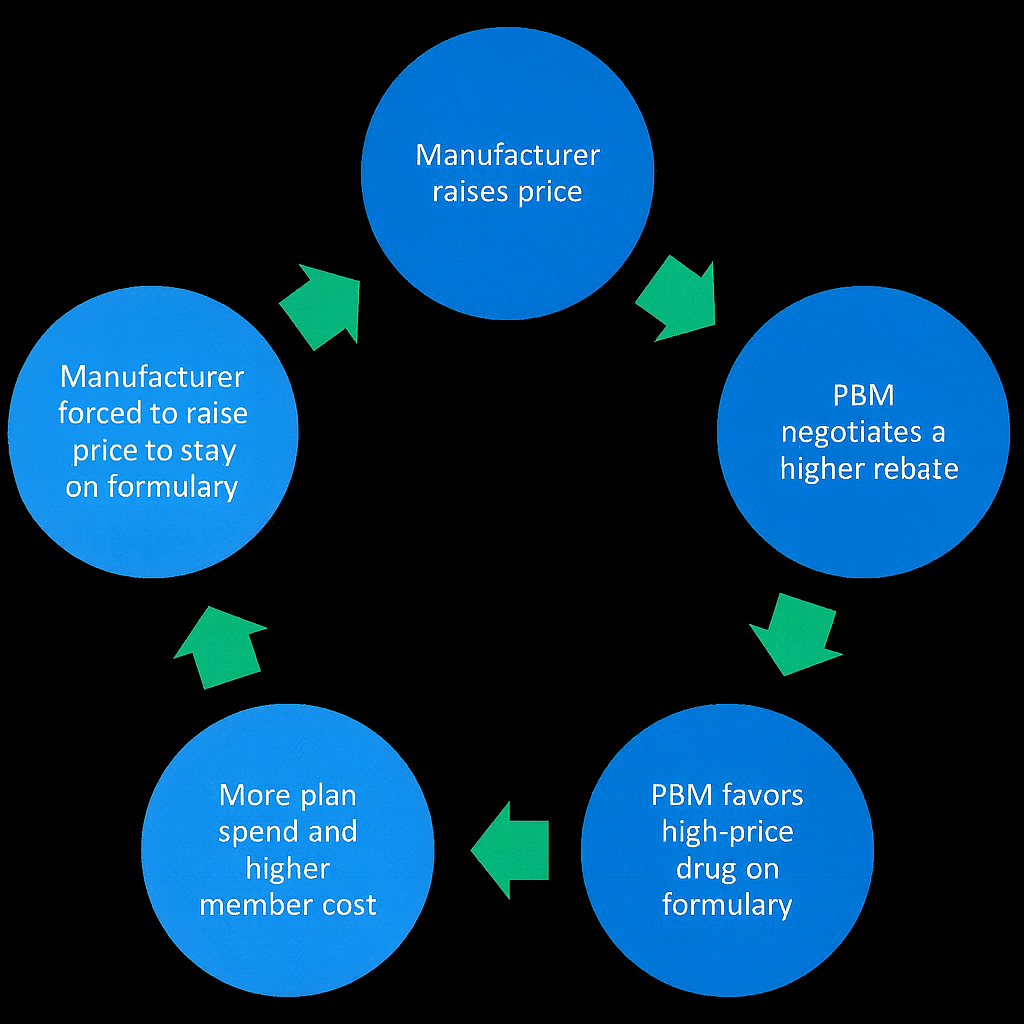
- Rebate-driven formulary changes: Some PBMs may pressure committees to favor high-rebate drugs even when lower-cost equivalents are equally effective. This practice shifts savings from the plan sponsor to the PBM.
- Manufacturer marketing: Drugmakers may inundate physicians or committee members with promotional materials that overstate benefits or underplay risks.
- Plan design overrides: Employers or insurers sometimes introduce benefit designs that favor drugs not aligned with the formulary’s intent.
- Member or prescriber appeals: When members or doctors appeal formulary exclusions based on personal preference rather than clinical necessity, consistent decision-making becomes difficult.
Each of these pressures threatens the committee’s independence and, by extension, the fiduciary duty employers owe their plan members.
How HR and Benefits Leaders Can Protect P&T Integrity
Protecting the committee’s work starts with strong governance and oversight. HR and finance leaders should see the P&T Committee as a safeguard for plan integrity, not a formality. The committee must operate independently from the PBM’s rebate and network teams, with members selected through a transparent process and governed by written bylaws that prevent conflicts of interest.
Documentation matters. Meeting minutes, voting records, and decision rationales should be retained and easily accessible. These records demonstrate fiduciary care and ensure that coverage decisions are based on objective evidence, not financial influence.
Employers also need to confirm that P&T decisions align with plan design yet remain insulated from rebate negotiations. When PBMs allow financial motives to shape clinical judgment, the process loses credibility.
Clear communication with plan members is equally critical. Employees deserve to know why certain drugs are covered and others are not. Transparency builds trust and minimizes confusion over cost-sharing or exclusions.
Lastly, benefits teams need regular training to understand formularies, drug tiers, and PBM reports. This knowledge helps them spot misalignment and reinforces the committee’s work. Strong governance, transparency, and education together ensure that the P&T Committee’s decisions protect both plan integrity and member health.
Practical Checklist: Safeguarding the P&T Process
- Verify the P&T Committee’s independence and review its bylaws annually.
- Require conflict-of-interest disclosures from all committee members.
- Audit a sample of formulary decisions each year to confirm documentation and rationale.
- Include P&T governance standards in PBM contracts and service-level agreements.
- Provide plan members with transparent communication about formulary updates.
Call to Action
Pharmacy and Therapeutics Committees are the quiet guardians of clinical and financial integrity in pharmacy benefits. Employers and HR leaders who understand their importance can prevent waste, avoid conflicts of interest, and keep members safe. Now is the time to review your PBM’s P&T governance structure, verify its independence, and ensure every formulary decision serves one goal: better care, cost-effectively.
Elevate your expertise in pharmacy benefits management with the Certified Pharmacy Benefits Specialist® (CPBS) program. Whether you’re an HR leader, finance executive, consultant, or pharmacist, this certification provides the in-depth knowledge and strategic insight needed to manage pharmacy benefits with confidence and cost efficiency. Earn up to twenty continuing education credits while advancing your fiduciary and professional competencies. The CPBS program is accredited by both SHRM and HRCI, making it a powerful addition to your professional development portfolio. Strengthen your career, deliver measurable results, and help your organization take control of pharmacy spend. Register today to join a growing network of professionals shaping the future of pharmacy benefits management.