Study Reveals Factors That Dissuade Commercial Plans From Covering Biosimilars [Weekly Roundup]
Study Reveals Factors That Dissuade Commercial Plans From Covering Biosimilars and other notes from around the interweb:
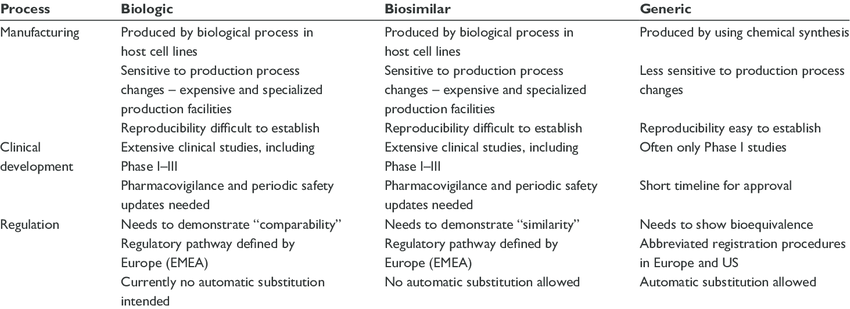
- Study Reveals Factors That Dissuade Commercial Plans From Covering Biosimilars. A recent study found factors that influence a commercial plan’s likelihood of placing coverage restrictions on biosimilars, including how many competitors are on the market, the prevalence of the drug indications, and the plan’s relationship with pharmacy benefit managers (PBMs). The study, published in BioDrugs, is the first to examine the characteristics associated with US commercial health plan biosimilar coverage. It also expanded on previous literature that found that biosimilars were preferred over their reference products in only 14% of coverage decisions and were less preferred in 33% of cases. The researchers used data on coverage decisions from the Tufts Medical Center Specialty Drug Evidence and Coverage database, cost-effectiveness evidence from the Tufts Medical Center Cost-Effectiveness Analysis Registry, and list prices from the Merative Micromedex RED BOOK. They identified 1181 coverage decisions through August 2021 regarding 19 commercially available biosimilars for 7 reference products and 28 indications.
- AHF Confronts Cigna CEO over PBM’s ‘Rapacious’ Greed. AIDS Healthcare Foundation (AHF), the world’s largest HIV/AIDS healthcare provider, sharply criticized health care behemoth Cigna today over its management of Express Scripts, the nation’s second largest Pharmacy Benefit Manager (PBM), which Cigna acquired in a 2018 merger. AHF’s criticism comes on the heels of a so-called “transparency” campaign Cigna and Express Scripts recently launched. In a letter to Cigna CEO David Cordani, AHF President Michael Weinstein details how Cigna, through its Express Scripts PBM, “…is ripping apart the healthcare system through its rapacious, self-serving, member-unfriendly practices…” Issues concerning AHF and hundreds of independent and mom-and-pop pharmacies nationwide include the following: Express Scripts (ESI) actively drives pharmacies out of its networks through reimbursements that don’t even cover a pharmacy’s drug costs, let alone the costs associated with dispensing the drugs and consulting with patients. This predatory practice is contributing to the bankruptcy of independent pharmacies and to the creation of pharmacy deserts, leaving members stranded.

- Florida is still battling the federal government over imported drugs. Gov. Ron DeSantis and then-Florida House Speaker Jose Oliva, R-Miami Lakes, made the drug-importation issue a priority in 2019, with lawmakers approving a plan to make imported drugs available in government programs such as Medicaid, the prison system and facilities run by the Department of Children and Families. At least initially, the state wants to import drugs to treat conditions such as HIV and AIDS, hepatitis C, diabetes, and mental illness, according to court documents. The state submitted a proposal in November 2020 to the Food and Drug Administration, which would need to approve the importation program. The proposal falls under what is known as the federal Section 804 Importation Program, or SIP
- What is transparency? Six things to look for in a PBM contract. If you don’t know the answer, they’re not transparent. PBMs aren’t incentivized to be transparent because they make money on drugs in many creative ways. So long as this remains true, their interests are not aligned with those of the employer or employees, and being transparent puts their business model at risk. For example, it’s an open secret that many PBMs make huge profits by negotiating “rebates” with drug manufacturers in the name of lowering the price of drugs. The truth is that those PBMs run a pay-to-play scheme, excluding from their formularies the drug manufacturers that don’t pay the rebates. The PBMs argue they are now passing most rebates received to employers to reduce drug costs. It should be no surprise that, at the same time rebate revenue has gone down for PBMs, they experienced a commensurate or greater increase in “admin fees” received from manufacturers for “processing rebates.” Whether you call it a rebate or an admin fee, it has the same effect: driving up wholesale drug prices and lining the PBM’s pocket at employer and patient expense. Another customary practice is “spread pricing,” where a PBM adds margin to the price they pay the pharmacy versus what they charge health plans and patients. Who keeps the spread? The PBMs, of course. And pharmacy owners, health plans, and health care consumers pay the price.