Building the In-house Pharmacy Benefit: Three considerations for the health system as plan sponsor
 As one of the largest employers in the healthcare industry, the challenges for hospitals are no different. More and more hospitals and health systems are considering building in-house outpatient pharmacies to combat rising costs, adherence issues and management issues surrounding their employee benefit programs while improving care, convenience and cost for employees as well. And while health systems are finding significant benefits when it comes to offering the ambulatory pharmacy benefit, success depends on proper planning in three important areas.
As one of the largest employers in the healthcare industry, the challenges for hospitals are no different. More and more hospitals and health systems are considering building in-house outpatient pharmacies to combat rising costs, adherence issues and management issues surrounding their employee benefit programs while improving care, convenience and cost for employees as well. And while health systems are finding significant benefits when it comes to offering the ambulatory pharmacy benefit, success depends on proper planning in three important areas.
Cost/benefit analysis.
Building an in-house pharmacy is a big commitment with a potentially bigger payoff. Doing so could help hospitals save 8 to 12 percent on the buy side, and employees are more likely to adhere to therapy plans if they have a convenient and cost-effective place to fill their prescriptions. The health and wellness of employees correlates directly to how much employers spend on healthcare. Plus, less sick time means happier, more productive employees – and the indirect costs of decreased productivity due to illness can significantly impact a company’s bottom line.
Build strategy and benefits planning.
Of course, building an outpatient pharmacy isn’t easy. In addition to determining cost, location, size and profitability, hospitals and health systems will need to identify the patient populations they want to target and then develop a business plan to maximize opportunities. A critical component of that business plan should be the integration of the hospital’s employee benefits into pharmacy operations.
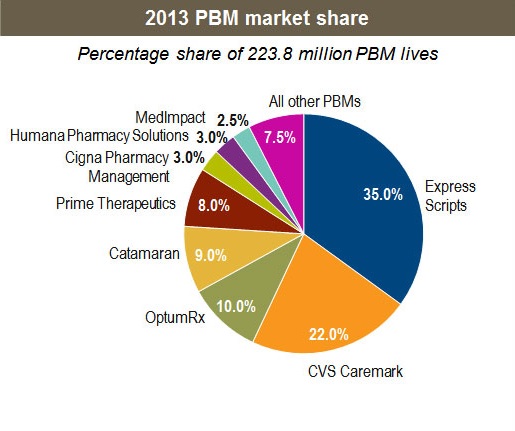
Pharmacy benefit managers (PBMs) can play a central role in administering pharmacy benefits on behalf of employer-sponsored plans. PBMs provide pharmacy benefits to about 200 million Americans. Traditionally, PBMs are responsible for prescription processing, claims filling, benefit plan design, drug formulary management, rebate and reimbursement administration and more. Given the prevalence and unique role of PBMs, most hospitals have an existing relationship with a PBM to administer their pharmacy benefit. The health system’s pharmacy business plan should account for partnering with a PBM to drive formulary compliance while promoting medication adherence.
Delivering value for employees.
In order for a hospital to leverage its in-house pharmacy to gain the greatest value for its employees, it is important to establish the pharmacy as the provider of choice. Considerations for positioning the health system as a healthcare destination for its employees include:
- How will the qualified, professional staff of pharmacists and pharmacy technicians thrive as part of the hospital’s team and the employee’s healthcare team?
- What collaborative care initiatives will the in-house pharmacy pursue to differentiate it as a preferred offering?
- How will the health system highlight and promote the excellent customer service and convenience of the in-house pharmacy?
- What is the best way to combine existing expertise with new resources to improve employee wellness?
- What other services (on-site delivery, education, OTC products, etc.) will the pharmacy offer?
- How will the HR/benefits team and pharmacy staff partner to position the pharmacy for success? Which team has ownership of various strategic initiatives?
Health systems are uniquely positioned to leverage their knowledge and resources to improve the health of employees. And though employee benefit costs are on the rise, building an in-house pharmacy can pay off for both the hospital and its employees. Implementing an in-house pharmacy is a significant undertaking. But it’s also a strategic investment that can save precious healthcare dollars.
By Amy Flowers