Because plan sponsors don’t know how to calculate how much money pharmacy benefit managers (PBM) make, it gives PBMs all the incentive they need to overcharge. How many businesses do you know want to cut their revenues in half? That’s why traditional pharmacy benefit managers, and their stakeholders, don’t offer a fiduciary standard of care and instead opt for hidden cash flow opportunities to generate their service fees. Want to learn more?
“Thank you, Tyrone, for this informative meeting.” David Wachtel, VP
“…Great presentation! I had our two partners at the presentation as well. Very informative.” Nolan Waterfall, Agent/Benefits Specialist
A snapshot of what you will learn during this 30-minute webinar:
Hidden cash flows in the PBM Industry
Basic to intermediate level PBM terminologies
Specialty pharmacy cost-containment strategies
Examples of drugs that you might be covering that are costing you
The #1 metric to measure when evaluating PBM cost performance
Understanding how PBMs make money and how much you pay them for their services is a key element in running an efficient pharmacy benefits program. Join us to learn more.
PSAOs Primed to Unlock Specialty Payor Contracts and other notes from around the interweb:
Federal Judge Rules Cheaper Drugs Can Be Imported From Canada. In a setback to the pharmaceutical industry, a federal judge has tossed a lawsuit that sought to prevent state governments from importing medicines from Canada. And the decision is likely to embolden more states to now consider the approach as they look to lower the cost of prescription drugs. The 26-page ruling noted that to have standing, plaintiffs must prove that they have suffered an “injury in fact,” that the injury is traceable to the defendants’ conduct, and that the injury is likely to be remedied by a favorable decision. And in two distinct aspects, the plaintiffs had no standing to bring the case against the federal agencies, Kelly ruled. The DC Circuit Court has struck a blow against the pharmaceutical lobbying group PhRMA and other plaintiffs’ attempt to stop states from importing drugs from Canada. Joined alongside public health group Partnership for Safe Medicines and advocacy group Council for Affordable Health Coverage, PhRMA was rebuffed by Judge Timothy Kelly, who dismissed the civil suit due to a lack of standing.
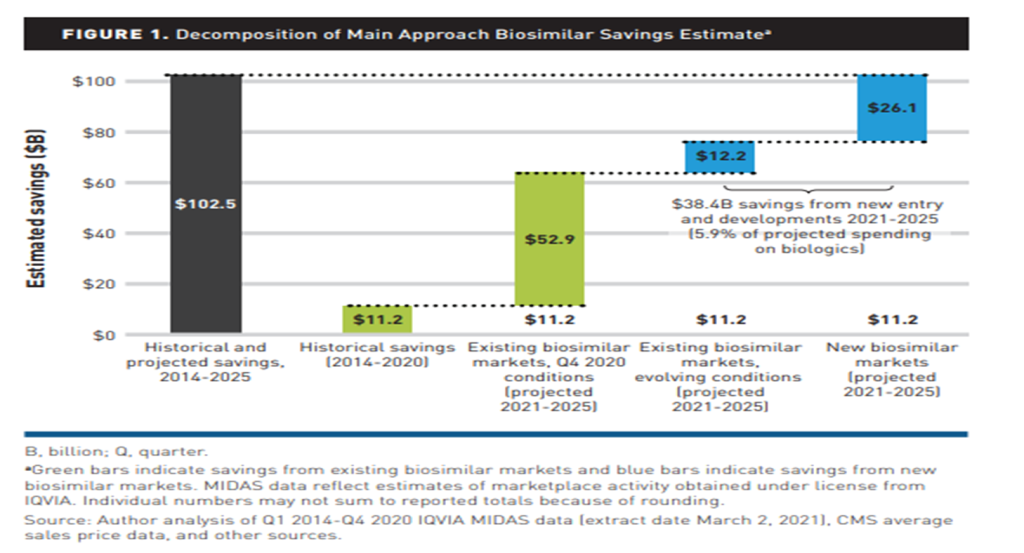
7 Key Facts About Biosimilars. When describing biosimilars to patients, remind them that in their simplest form, medications are chemical structures, with some comprising simple, small molecules or pieces, while others are more complex. Biosimilars are made of complex chemical structures. Because biosimilars are complex medications, there are often products that treat complex conditions, such as insulin for diabetes and other biosimilars for conditions, such as multiple sclerosis or psoriasis. Many biosimilars are dispensed by specialty pharmacies, which provide medications that are typically expensive for medical conditions that are intricate and often difficult to treat. The FDA approved the first biosimilar, Zarxio (filgrastim-sndz) on March 6, 2015, for the reference product Neupogen. Zarxio was approved for all indications included on the reference product’s label, which is not the case for all biosimilars.
States, not Federal Government, Are Moving to Tighten Regulation of PBMs. The action on PBMs has devolved to the states partly because a 2020 U.S. Supreme Court decision, said leaders with the National Academy for State Health Policy. In Rutledge v Pharmaceutical Care Management Association, the court upheld an Arizona law that required PBMs to pay pharmacies no less than their acquisition costs for prescription drugs. The court indicated the Arizona law was not preempted by Employee Retirement Income Security Act (ERISA), a federal law that sets standards for retirement and health benefits. The decision in the case gives states the ability to regulate healthcare costs, including health plan contractors. In 2022, 135 bills concerning PBMs were introduced in state legislatures, according to the National Academy for State Health Policy’s tracker. Most are still working their way through various committees, and some have failed to make any headway. The 19 bills that have been signed into law provide a starting point to address the undue influence that PBMs have over pharmacies and drug pricing, say the industry’s critics.
PSAOs Primed to Unlock Specialty Payor Contracts. A Pharmacy Services Administrative Organization (PSAO) is a third-party organization that provides administrative and business support services to independent pharmacies. PSOAs negotiate contracts with pharmacy benefit managers (PBMs) and health plans on behalf of their member pharmacies to ensure fair reimbursement rates and optimal drug pricing. For local and regional health-system specialty pharmacies, the phrase “out of network” often is a painful reminder that many of their specialty patients must go to outside pharmacies or mail-service providers to receive their essential medications. It’s a persistent challenge to health systems’ integrated specialty care model, but one that may be easier to overcome after the recent launches of Pharmacy Services Administrative Organizations (PSAOs) and other alliances that seek to open specialty contracts to more players. Unlocking payor networks remains a challenge, even as mounting evidence shows the benefits of integrated care for patients with cancer and other complex and difficult-to-treat conditions.
The definition of specialty drug varies which makes the 10 things to know about biosimilar drugs that much more relevant. In fact, the FDA does not define drugs as ‘Specialty’. The APhA (American Pharmacists Association) describes specialty medications as having some or all the following key characteristics:
High cost (often more than $10,000 per patient per year)
Special handling / Administration (refrigerate/frozen, drug delivery devices)
Frequent dosing adjustments required
Limited/Exclusive distribution by manufacturer
Government required REMS (risk evaluation mitigation strategies) program
Treats a complex/chronic condition that could lead to life threatening situations if left untreated
Advanced patient training required in administration / usage of drug
Biologics
Humira (adalimumab) is a biological drug that belongs to a class of medications called TNF inhibitors. It is used to treat a variety of autoimmune diseases, including rheumatoid arthritis, psoriasis, Crohn’s disease, ulcerative colitis, and ankylosing spondylitis. Humira works by blocking the action of tumor necrosis factor-alpha (TNF-alpha), a protein that plays a role in inflammation. By reducing the activity of TNF-alpha, Humira helps to reduce inflammation and improve symptoms of autoimmune diseases.
Humira is administered as a subcutaneous injection and is typically given once every two weeks or once a week, depending on the condition being treated. The dosage and frequency of administration may be adjusted based on the patient’s response to treatment. Humira is one of the most widely used biological drugs, with sales of over $20 billion in 2020. It was first approved by the US Food and Drug Administration (FDA) in 2002 and has since been approved for use in over 100 countries.
While Humira is generally considered safe and effective, it can have side effects, including increased risk of infection, allergic reactions, and increased risk of certain types of cancer. Patients taking Humira should be closely monitored for side effects and should report any symptoms to their healthcare provider. Humira is also one of the most expensive drugs on the market, with an average cost of over $5,000 per month. However, the availability of biosimilar versions of Humira will help to reduce the cost of treatment for many patients. Here are 10 things to know about biosimilar drugs.
Biosimilars are biological drugs that are similar to a reference biological drug that has already been authorized for use.
Biosimilars are made using living cells and can be more complex than traditional chemical drugs, which are made from chemical compounds.
Biosimilars are not identical to the reference drug, but are highly similar in terms of quality, safety, and efficacy.
Biosimilars can be used to treat a variety of diseases, including cancer, autoimmune disorders, and chronic inflammatory conditions.
The development of biosimilars requires extensive testing and clinical trials to demonstrate that they are safe and effective.
Biosimilars are typically less expensive than the reference biological drug, which can help to reduce healthcare costs and increase access to treatment.
The approval process for biosimilars is different from traditional generic drugs and involves a detailed review of the manufacturing process and clinical trial data.
Biosimilars are regulated by the same agencies that oversee the approval of the reference biological drug, such as the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA).
Biosimilars may have minor differences in their structure or composition compared to the reference drug, but these differences do not affect their safety or efficacy.
Biosimilars are becoming more widely used around the world, as more manufacturers seek to develop and market these drugs to meet the growing demand for affordable biologic therapies.
Amjevita (adalimumab-atto) is a biosimilar drug to Humira (adalimumab). It was approved by the US Food and Drug Administration (FDA) in 2016 for the treatment of several autoimmune diseases, including rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn’s disease, ulcerative colitis, and plaque psoriasis. Today, Amjevita is available in pharmacies at discounts as high as 55% off AWP.
Employer-sponsored plans pay up to 3,350 percent higher than Medicare for commonly used medications and other notes from around the interweb:
Federal Judge Rules Cheaper Drugs Can Be Imported From Canada. In a setback to the pharmaceutical industry, a federal judge has tossed a lawsuit that sought to prevent state governments from importing medicines from Canada. And the decision is likely to embolden more states to now consider the approach as they look to lower the cost of prescription drugs. The 26-page ruling noted that to have standing, plaintiffs must prove that they have suffered an “injury in fact,” that the injury is traceable to the defendants’ conduct, and that the injury is likely to be remedied by a favorable decision. And in two distinct aspects, the plaintiffs had no standing to bring the case against the federal agencies, Kelly ruled. The DC Circuit Court has struck a blow against the pharmaceutical lobbying group PhRMA and other plaintiffs’ attempt to stop states from importing drugs from Canada. Joined alongside public health group Partnership for Safe Medicines and advocacy group Council for Affordable Health Coverage, PhRMA was rebuffed by Judge Timothy Kelly, who dismissed the civil suit due to a lack of standing.
What Johnson & Johnson’s Lawsuit Against SaveOnSP Means for Drug Manufacturers and Plan Sponsors. On January 25, 2023, the Court in Johnson & Johnson v. SaveOnSP[1] dismissed SaveOnSP’s motion to dismiss, allowing Johnson & Johnson’s (“JNJ”) claims to proceed. The Court’s recent order is a significant development, especially as several manufacturers following the JNJ’s lawsuit have updated the terms and conditions of their copay assistance programs to restrict (or exclusively carving out) copay maximizer such as SaveOnSP from their programs. JNJ alleges that SaveOnSP inflated patients’ copays by reclassifying drugs to avoid copay limits and annual out-of-pocket limits mandated by the US Affordable Care Act (“ACA”) to coerce patients into enrolling in the SaveOnSP program and bill the artificially inflated copays to JNJ’s copay assistance program. JNJ’s complaint also alleges that SaveOnSP worked in partnership with major PBM Express Scripts (“ESI”) and ESI’s specialty pharmacy Accredo Health Group to operate the program and, in turn, maximize its profits at the expense of both patients and JNJ.
States, not Federal Government, Are Moving to Tighten Regulation of PBMs. The action on PBMs has devolved to the states partly because a 2020 U.S. Supreme Court decision, said leaders with the National Academy for State Health Policy. In Rutledge v Pharmaceutical Care Management Association, the court upheld an Arizona law that required PBMs to pay pharmacies no less than their acquisition costs for prescription drugs. The court indicated the Arizona law was not preempted by Employee Retirement Income Security Act (ERISA), a federal law that sets standards for retirement and health benefits. The decision in the case gives states the ability to regulate healthcare costs, including health plan contractors. In 2022, 135 bills concerning PBMs were introduced in state legislatures, according to the National Academy for State Health Policy’s tracker. Most are still working their way through various committees, and some have failed to make any headway. The 19 bills that have been signed into law provide a starting point to address the undue influence that PBMs have over pharmacies and drug pricing, say the industry’s critics.
For commonly used medications, employer-sponsored plans pay up to 3,350 percent higher than Medicare. According to a research letter published in JAMA Health Forum and based on data from employer-sponsored insurance, Medicare pays substantially lower rates for medications prescribed by doctors. From 2016 through 2020, researchers at the Healthcare Cost Institute examined the per-unit costs of the 10 most costly and 10 most often used prescription medications. Employer-sponsored insurance paid costs that were up to 3,350 percent more than Medicare for the most frequently used medications. Employer-sponsored insurance paid 20 times more for ondansetron and paid 30 times more for midazolam than Medicare did for the same medication. The researchers discovered that employer-sponsored plans did not pay as high markups for the most expensive medications. At the top end, markups were 54% higher than Medicare, and several medications were covered at rates comparable to Medicare by employer-sponsored plans.
Federal Judge Rules Cheaper Drugs Can Be Imported From Canada and other notes from around the interweb:
Federal Judge Rules Cheaper Drugs Can Be Imported From Canada. In a setback to the pharmaceutical industry, a federal judge has tossed a lawsuit that sought to prevent state governments from importing medicines from Canada. And the decision is likely to embolden more states to now consider the approach as they look to lower the cost of prescription drugs. The 26-page ruling noted that to have standing, plaintiffs must prove that they have suffered an “injury in fact,” that the injury is traceable to the defendants’ conduct, and that the injury is likely to be remedied by a favorable decision. And in two distinct aspects, the plaintiffs had no standing to bring the case against the federal agencies, Kelly ruled. The DC Circuit Court has struck a blow against the pharmaceutical lobbying group PhRMA and other plaintiffs’ attempt to stop states from importing drugs from Canada. Joined alongside public health group Partnership for Safe Medicines and advocacy group Council for Affordable Health Coverage, PhRMA was rebuffed by Judge Timothy Kelly, who dismissed the civil suit due to a lack of standing.
What Johnson & Johnson’s Lawsuit Against SaveOnSP Means for Drug Manufacturers and Plan Sponsors. On January 25, 2023, the Court in Johnson & Johnson v. SaveOnSP[1] dismissed SaveOnSP’s motion to dismiss, allowing Johnson & Johnson’s (“JNJ”) claims to proceed. The Court’s recent order is a significant development, especially as several manufacturers following the JNJ’s lawsuit have updated the terms and conditions of their copay assistance programs to restrict (or exclusively carving out) copay maximizer such as SaveOnSP from their programs. JNJ alleges that SaveOnSP inflated patients’ copays by reclassifying drugs to avoid copay limits and annual out-of-pocket limits mandated by the US Affordable Care Act (“ACA”) to coerce patients into enrolling in the SaveOnSP program and bill the artificially inflated copays to JNJ’s copay assistance program. JNJ’s complaint also alleges that SaveOnSP worked in partnership with major PBM Express Scripts (“ESI”) and ESI’s specialty pharmacy Accredo Health Group to operate the program and, in turn, maximize its profits at the expense of both patients and JNJ.
States, not Federal Government, Are Moving to Tighten Regulation of PBMs. The action on PBMs has devolved to the states partly because a 2020 U.S. Supreme Court decision, said leaders with the National Academy for State Health Policy. In Rutledge v Pharmaceutical Care Management Association, the court upheld an Arizona law that required PBMs to pay pharmacies no less than their acquisition costs for prescription drugs. The court indicated the Arizona law was not preempted by Employee Retirement Income Security Act (ERISA), a federal law that sets standards for retirement and health benefits. The decision in the case gives states the ability to regulate healthcare costs, including health plan contractors. In 2022, 135 bills concerning PBMs were introduced in state legislatures, according to the National Academy for State Health Policy’s tracker. Most are still working their way through various committees, and some have failed to make any headway. The 19 bills that have been signed into law provide a starting point to address the undue influence that PBMs have over pharmacies and drug pricing, say the industry’s critics.
Summit County sues pharmacy benefits managers over opioid crisis. Governments, insurers, or employers typically hire pharmacy benefit managers to facilitate prescription drug programs, with the goal of reducing costs for the insured. The lawsuit, however, accuses the companies of doing the opposite. It alleges the businesses colluded with manufacturers to make opioids more available for pain treatment and by ignoring clear warning signs of addiction in patients. The companies did so to increase profits, the lawsuit said. “Whether by colluding with manufacturers to make opioids more available as a form of pain treatment or by ignoring the mounting evidence of addiction and misuse in their own claims data, [pharmacy benefits managers’] role in creating and sustaining the opioid epidemic is largely hidden from public scrutiny but nevertheless facilitated the reckless promotion of opioids by manufacturers, the oversupply of opioid shipments by distributors and the irresponsible dispensing of prescription opioids by numerous pharmacies,” the lawsuit said.
A specialty drug is a type of medication that is used to treat complex or chronic conditions and requires specialized administration, handling, and monitoring. These drugs are often high-cost (⁓$10000/yr.) and may require special storage or handling conditions. Examples of specialty drugs include biologic medications used to treat autoimmune disorders, cancer treatments, and intravenous medications for severe infections or pain management.
Specialty drugs are often used for rare or complex medical conditions and may require close monitoring and management by healthcare professionals. They may also have unique side effects and require specialized administration, such as intravenous infusions or subcutaneous injections.
Because of their high cost and specialized nature, the management of specialty drugs can be a challenge for patients, healthcare providers, and insurance providers. In some cases, patients may require prior authorization or other utilization management techniques to ensure that these drugs are used appropriately and cost-effectively. Here are 10 ways employers can effectively manage the cost of specialty drugs.
Partner with a radically transparent or fiduciary pharmacy benefit manager (PBM): PBMs specialize in managing prescription drug costs and can help negotiate lower prices for specialty drugs.
Encourage the use of generic and biosimilar options: Encouraging employees to use generic and biosimilar versions of specialty drugs can help reduce costs.
Implement a value-driven formulary management program: A value-driven formulary management program allows an employer to benefit from efficiency or safety and outcomes at the lowest net cost. Concisely, value-driven formularies help reduce costs for specialty drugs. In rebate-driven formularies, high-cost drugs create big earnings for PBMs that don’t have a legal duty to contain its clients costs. How motivated is your PBM to manage the formulary to lowest net cost? A generic dispense ratio (GDR) < 85% is an indication your PBM is not motivated much at all to deliver lowest net cost.
Negotiate with pharmaceutical manufacturers: Unions, coalitions, and large employers (Fortune 100) can negotiate directly with pharmaceutical manufacturers or health plans to include cost-saving measures for specialty drugs.
Leverage mail-order pharmacy efficiencies: Mail-order pharmacies often have lower prices for prescription drugs, including specialty medications.
Offer a medication therapy management (MTM) program: Encouraging employees to engage in preventive care and effectively manage chronic conditions can reduce the need for expensive specialty drugs.
Implement a reference-based pricing program: This program sets a maximum payment for certain drugs, which can help control costs for specialty drugs.
Provide educational resources: Educating employers and employees about the cost of specialty drugs and available cost-saving options can help them make informed decisions.
Encourage the use of patient assistance programs: Employers can educate employees about the availability of patient assistance programs offered by pharmaceutical companies, which can help cover the cost of specialty drugs.
Consider alternative treatment options: Employers can encourage the use of alternative treatment options, such as physical therapy or over-the-counter medications, which may be more cost-effective than specialty drugs.
There are thirty-two teams in the National Football League (NFL). The Super Bowl is the championship game of the National Football League (NFL), the highest level of professional American football in the United States. It is considered one of the biggest annual sporting events in the world. The Super Bowl is the reward for two teams who are better in the sport than the other 30 teams. The Kansas City Chiefs beat the Philadelphia Eagles yesterday in the Super Bowl. The Chiefs won the game because they executed better than the Eagles.
Register for CPBS today!
It’s important to note I’m not sharing any secret sauce with 10 Ways Employers Can Effectively Manage the Cost of Specialty Drugs. Yet, there are PBMs which execute better than others. Thirty-two teams play American football but two played it better than all the others. The same is true in pharmacy benefits management.
The buyer (plan sponsor) needs to be aware of the competitive market and their capacity to drive disclosure of information on services that are important to them, in addition to what they hope to accomplish in their relationship with their PBM. A trained eye with firsthand understanding of the purchaser’s benefit and disclosure objectives will be more efficient in evaluating transparency. Buyers of PBM services who are knowledgeable and sophisticated are the best advocates for radical transparency and lowest net cost.
What Johnson & Johnson’s Lawsuit Against SaveOnSP Means for Drug Manufacturers and Plan Sponsors and other notes from around the interweb:
Pharmacy Benefits Manager Refuses to Provide Requested Data to State Auditor’s Office. On April 30, 2021, state lawmakers passed House Bill 1004 which required the State Auditor’s Office to hire a third-party contractor to conduct a performance audit on the prescription drug coverage of NDPERS. The third-party contractor hired was Myers and Stauffer. The reason a third-party contractor would be required for this audit was because of the complex and specialized nature of the report. NDPERS is the organization that administers benefits to state employees. One of those benefits is healthcare. Sanford Health is the entity that provides healthcare to state employees. Sanford contracts with a third-party prescription benefits manager to manage pharmacy benefits for state employees. Their main responsibility is processing and paying prescription drug claims. They also negotiate discounts and rebates with drug manufacturers, contract with pharmacies, and maintain drug formularies.
What Johnson & Johnson’s Lawsuit Against SaveOnSP Means for Drug Manufacturers and Plan Sponsors. On January 25, 2023, the Court in Johnson & Johnson v. SaveOnSP[1] dismissed SaveOnSP’s motion to dismiss, allowing Johnson & Johnson’s (“JNJ”) claims to proceed. The Court’s recent order is a significant development, especially as several manufacturers following the JNJ’s lawsuit have updated the terms and conditions of their copay assistance programs to restrict (or exclusively carving out) copay maximizer such as SaveOnSP from their programs. JNJ alleges that SaveOnSP inflated patients’ copays by reclassifying drugs to avoid copay limits and annual out-of-pocket limits mandated by the US Affordable Care Act (“ACA”) to coerce patients into enrolling in the SaveOnSP program and bill the artificially inflated copays to JNJ’s copay assistance program. JNJ’s complaint also alleges that SaveOnSP worked in partnership with major PBM Express Scripts (“ESI”) and ESI’s specialty pharmacy Accredo Health Group to operate the program and, in turn, maximize its profits at the expense of both patients and JNJ.
Why Now Is the Time for Health Plans to Take Control of Pharmacy Benefits. It’s worth belaboring the point: PBMs are under the watchful eye of state and federal governments. The PBM of the future isn’t a gas-guzzling, polluting SUV, for example, it is an efficient, state-of-the-art, fully customizable electric vehicle. It is regulatory compliant and uses the best technology to ensure equitable pricing methodology, financial value, and great member experience. Instead of shrouding drug pricing in secrecy, new PBM business models rely on transparency. The best way to create an efficient and fair market is to allow both the buy and sell sides of the transaction to communicate freely about how drug prices are set, rebates, and other essential information. On the compliance side, plan sponsors must recognize and understand how their health plan drives revenue for their benefits brokers and consultants (e.g., are they compensated for recommendations on pharmacy benefits or any other aspect of health benefits?). The Consolidated Appropriations Act of 2021 places new fiduciary responsibilities on entities that provide health benefits, and plan sponsors must ask their broker or consultant to disclose how they’re compensated.
Summit County sues pharmacy benefits managers over opioid crisis. Governments, insurers, or employers typically hire pharmacy benefit managers to facilitate prescription drug programs, with the goal of reducing costs for the insured. The lawsuit, however, accuses the companies of doing the opposite. It alleges the businesses colluded with manufacturers to make opioids more available for pain treatment and by ignoring clear warning signs of addiction in patients. The companies did so to increase profits, the lawsuit said. “Whether by colluding with manufacturers to make opioids more available as a form of pain treatment or by ignoring the mounting evidence of addiction and misuse in their own claims data, [pharmacy benefits managers’] role in creating and sustaining the opioid epidemic is largely hidden from public scrutiny but nevertheless facilitated the reckless promotion of opioids by manufacturers, the oversupply of opioid shipments by distributors and the irresponsible dispensing of prescription opioids by numerous pharmacies,” the lawsuit said.
A pharmacy benefit manager (PBM) pass-through is a pricing arrangement in which the PBM does not retain any portion of the spread which is the difference between the reimbursement it receives from the payer and the cost of the drug it pays to the pharmacy or refunds paid by a rebate aggregator. Instead, the full spread is passed on to the pharmacy and refunds to the employer. This arrangement allows for increased transparency and helps to control drug costs for payers and patients. When unpacking the concept of pass-through pharmacy benefit managers consider these benefits and challenges.
Cost savings: A pass-through PBM can help employers reduce their overall drug costs by passing on the full spread between the reimbursement received from the payer and the cost of the drug to the pharmacy.
Improved transparency: A pass-through PBM provides increased transparency in pricing and reimbursement, allowing employers to better understand and manage their drug costs.
Increased negotiating power: By eliminating the PBM’s profit margin, a pass-through PBM provides employers with greater negotiating power when it comes to securing favorable prices for drugs.
Better alignment of incentives: With a pass-through PBM, the incentives of the PBM are aligned with the employer’s goals of controlling drug costs, as the PBM does not benefit from higher drug prices.
Improved patient outcomes: A pass-through PBM can help improve patient outcomes by ensuring that patients have access to the most appropriate and cost-effective medications. This can also lead to improved employee health and productivity, which can benefit the employer.
Challenges
Retention of rebates or discounts received from drug manufacturers: If a PBM retains any portion of rebates or discounts received from drug manufacturers, it cannot be considered a true pass-through PBM.
Undisclosed management fees: If a PBM hides management fees, it may not be considered a pass-through PBM as these fees increase the costs passed on to the employer. In pharmacy benefits management, these management fees are referred to as earnings after cash disbursements (EACD).
Misuse of the spread: If a PBM misuses the spread by using it for purposes other than covering its administrative costs, it cannot be considered a pass-through PBM.
Steering patients to higher-cost drugs: If a PBM steers patients to higher-cost drugs to increase the spread, ingredient cost or rebate, it cannot be considered a pass-through PBM.
Lack of transparency in pricing and reimbursement: If a PBM does not provide clear and transparent information on pricing and reimbursement, it may not be considered a pass-through PBM. This lack of transparency makes it difficult for pharmacies to accurately determine the cost of drugs and determine if they are receiving a fair price.
Management fees are the PBM’s cash balance after bills have been paid. Those bills include but are not limited to ingredient costs, dispensing fees, and refunds or rebates. Two things are required for a PBM to be considered pass-through; disclosure of management fees and the data necessary to verify the accuracy of management fees paid to the PBM. High management fees are paid when a PBM profits from ingredient cost and rebate spreads. Exorbitant management fees are paid when employers don’t know what their management fee (EACD) is.
PBMs know what employers want to see so they give it to them. Slide decks, proposals, and conversations all point to pass-through business models. How those same PBMs behave once the group goes live more closely resembles rent-seeking. Unpacking the concept of pass-through pharmacy benefit managers is not without its challenges. Consultants and HR must be astute in evaluating PBM contract language, for instance. A pass-through PBM will share its management fee and the data for verification. If a PBM is unwilling to share its management fee and provide the data necessary to verify accuracy, assume it is hiding something.
Chelsea Handler ‘didn’t know’ she was on Ozempic and other notes from around the interweb:
Health plan fiduciary breaches persist under CAA. The Consolidated Appropriations Act of 2021 (CAA) is the most significant compliance challenge employers have faced since the Affordable Care Act. Benefit advisers who serve the health and welfare side of our industry no doubt will need to continue paying close attention to this landmark legislation on behalf of their employer clients. New requirements are now in effect. They include the review of plan contracts and removal of all “gag clauses;” determination of “reasonableness” for vendor fees and services; prescription drug reporting for plan years 2020, 2021 and 2022; and analysis of parity between medical and mental health coverage. Failing to comply with these requirements leaves employers at risk of incurring fines and facing class-action lawsuits. But most organizations are still in the dark, believing their broker or TPA will handle compliance on their behalf, or that it’s simply “no big deal.”
Chelsea Handler ‘Didn’t Know’ She Was on Ozempic, Says Her Doctor ‘Just Hands It Out to Anybody’. Chelsea Handler talked about Ozempic being used for weight loss in Hollywood circles — and shared her own experience — during her appearance on Call Her Daddy. The comedian, 47, sat down with host Alex Cooper for an intimate conversation on the podcast, where she opened up about unknowingly being prescribed Ozempic, intended to treat Type 2 diabetes. “So, my anti-aging doctor just hands it out to anybody,” Handler admitted. “I didn’t even know I was on it. She said, ‘If you ever want to drop five lbs., this is good.’ However, the medication is not intended for people who need to lose just 5 lbs. Ozempic, or its counterpart Wegovy for people with obesity, works in the brain, and shifts the person’s fat mass set point, Dr. Ania Jastreboff, M.D., PhD., and an obesity medicine physician scientist at Yale University told PEOPLE. Further, the drug needs to be taken at a low dose at the beginning, and slowly increased over time. Chandler says she gave herself a dose after a vacation. “I came back from a vacation, and I injected myself with it. I went to lunch with my girlfriend a few days later, and she was like, ‘I’m not really eating anything. I’m so nauseous, I’m on Ozempic,'” she recalled. “And I was like, ‘I’m kind of nauseous too.’ But I had just come back from Spain and was jet-lagged.” Handler then said her friend asked if she was sure she wasn’t on Ozempic before sharing that she was just “on semaglutide.” “That’s Ozempic,” her friend explained.
Why Now Is the Time for Health Plans to Take Control of Pharmacy Benefits. It’s worth belaboring the point: PBMs are under the watchful eye of state and federal governments. The PBM of the future isn’t a gas-guzzling, polluting SUV, for example, it is an efficient, state-of-the-art, fully customizable electric vehicle. It is regulatory compliant and uses the best technology to ensure equitable pricing methodology, financial value, and great member experience. Instead of shrouding drug pricing in secrecy, new PBM business models rely on transparency. The best way to create an efficient and fair market is to allow both the buy and sell sides of the transaction to communicate freely about how drug prices are set, rebates, and other essential information. On the compliance side, plan sponsors must recognize and understand how their health plan drives revenue for their benefits brokers and consultants (e.g., are they compensated for recommendations on pharmacy benefits or any other aspect of health benefits?). The Consolidated Appropriations Act of 2021 places new fiduciary responsibilities on entities that provide health benefits, and plan sponsors must ask their broker or consultant to disclose how they’re compensated.
Summit County sues pharmacy benefits managers over opioid crisis. Governments, insurers, or employers typically hire pharmacy benefit managers to facilitate prescription drug programs, with the goal of reducing costs for the insured. The lawsuit, however, accuses the companies of doing the opposite. It alleges the businesses colluded with manufacturers to make opioids more available for pain treatment and by ignoring clear warning signs of addiction in patients. The companies did so to increase profits, the lawsuit said. “Whether by colluding with manufacturers to make opioids more available as a form of pain treatment or by ignoring the mounting evidence of addiction and misuse in their own claims data, [pharmacy benefits managers’] role in creating and sustaining the opioid epidemic is largely hidden from public scrutiny but nevertheless facilitated the reckless promotion of opioids by manufacturers, the oversupply of opioid shipments by distributors and the irresponsible dispensing of prescription opioids by numerous pharmacies,” the lawsuit said.
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.